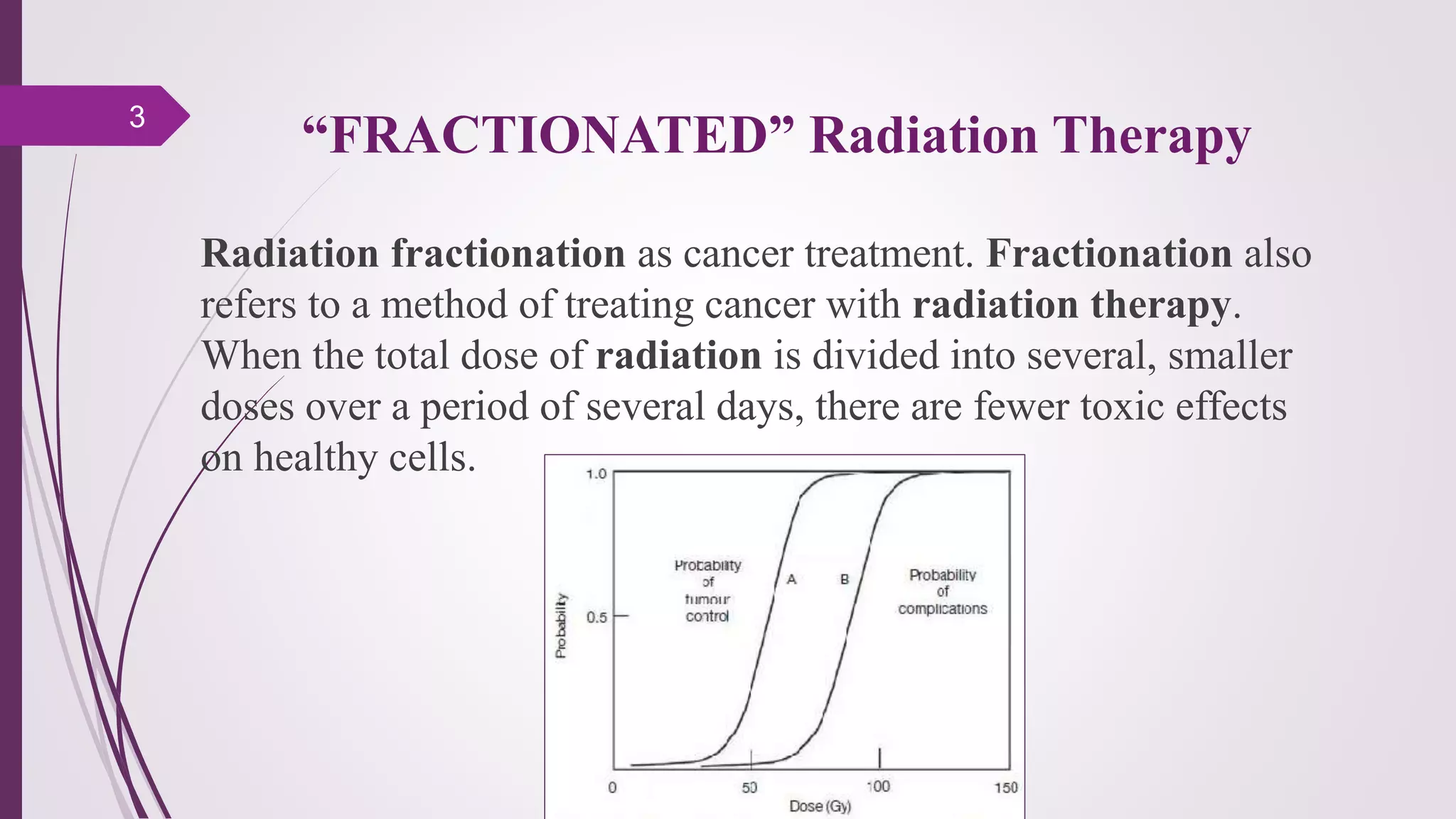
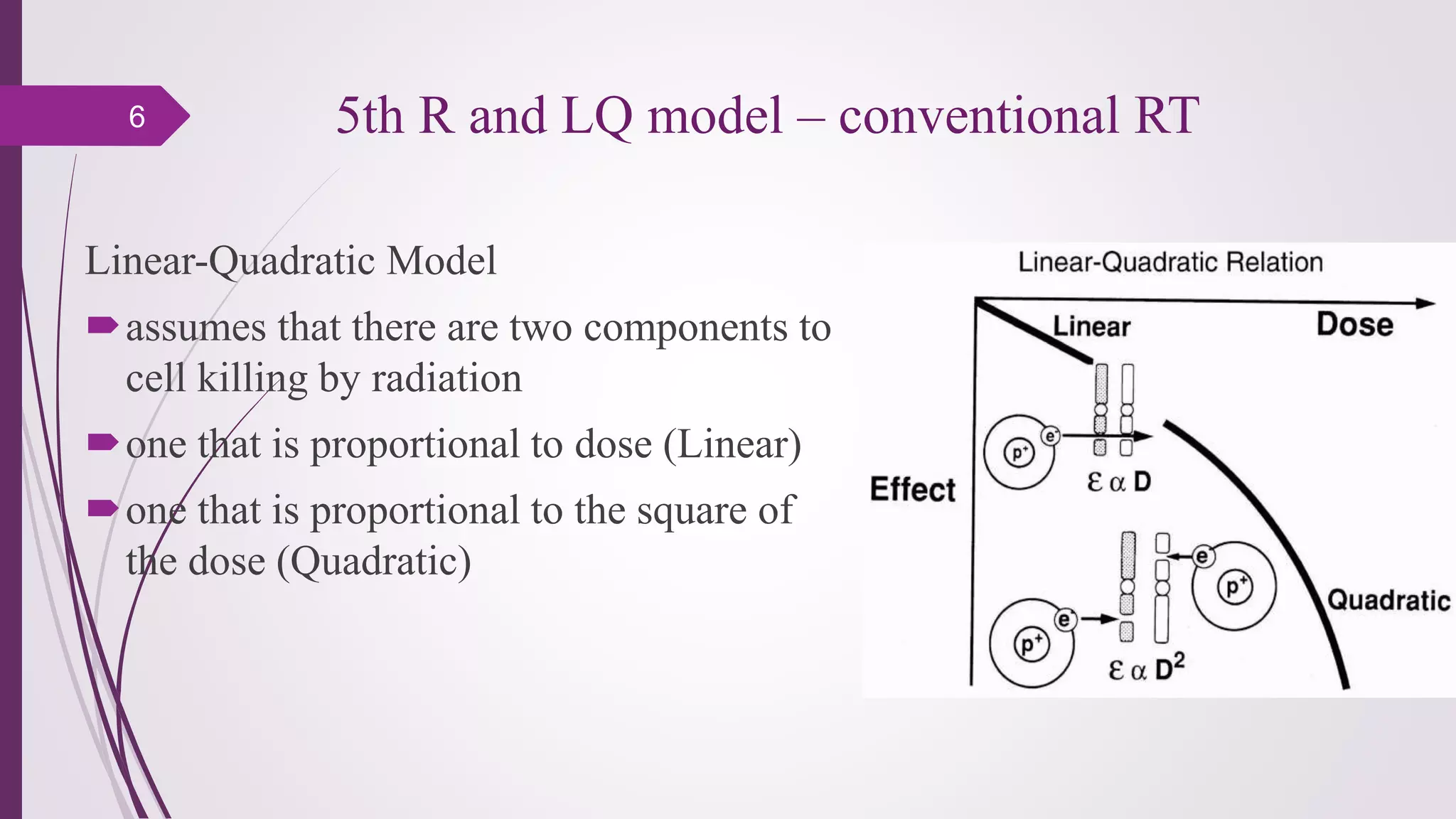
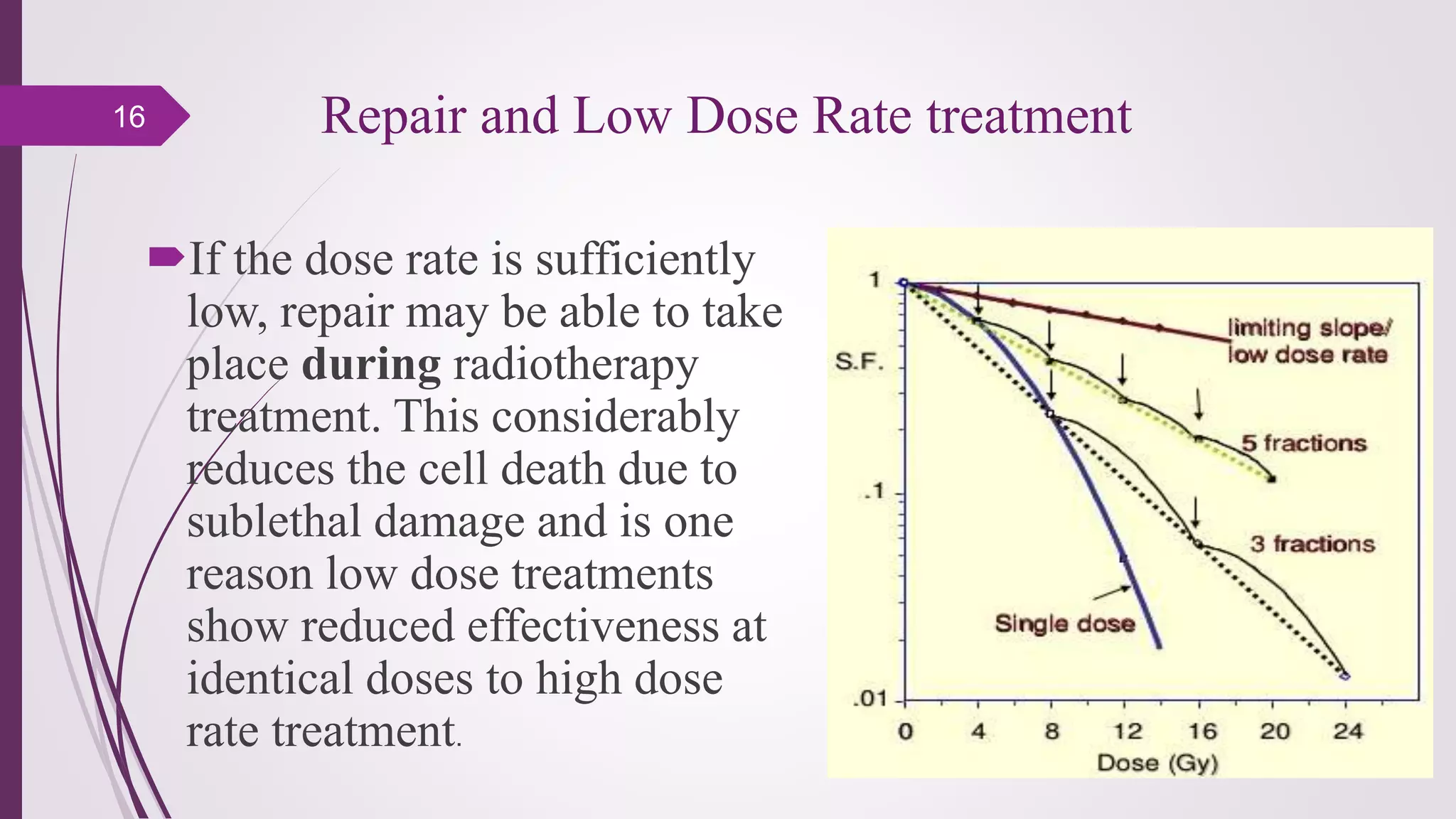
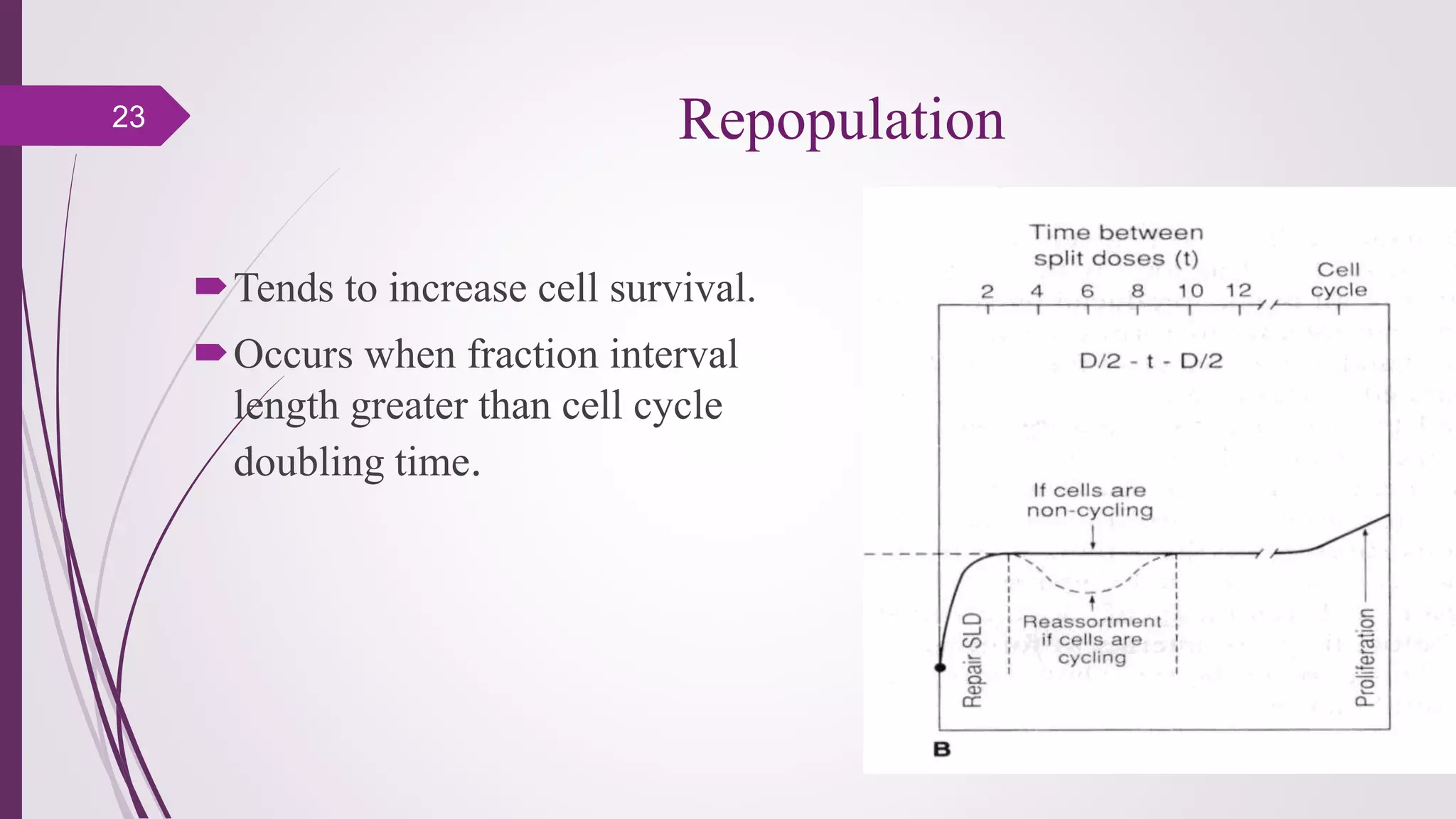
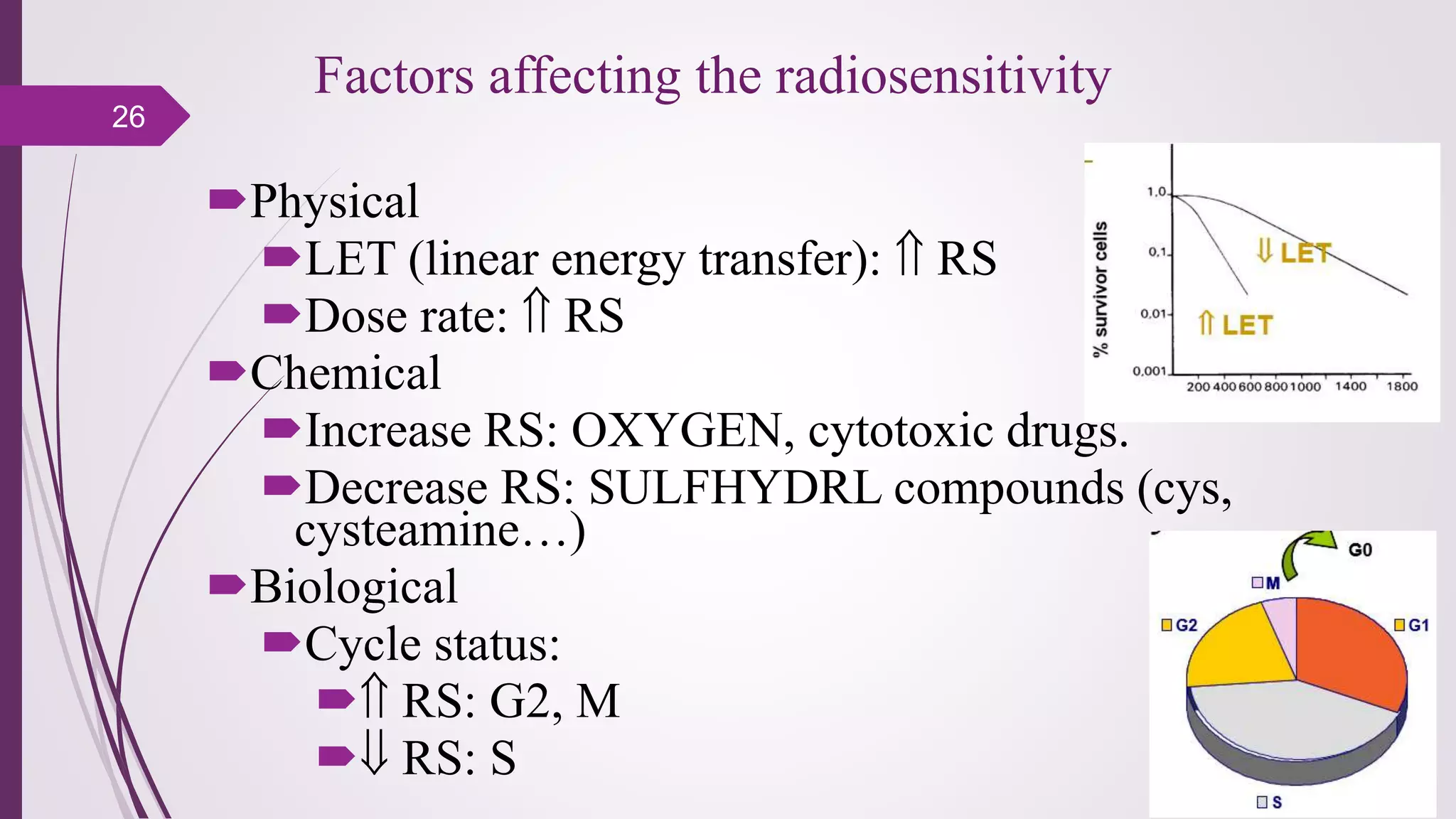
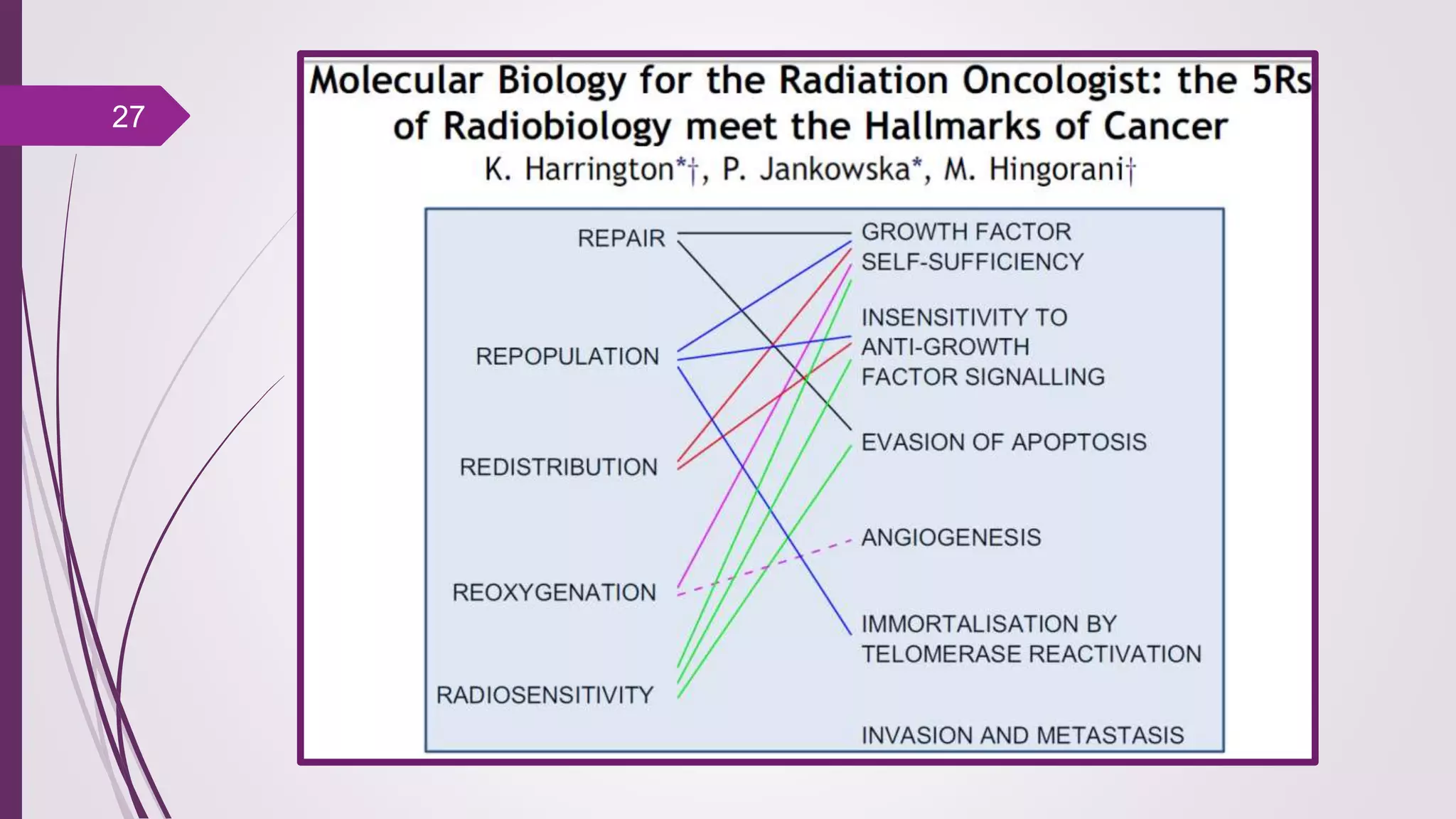
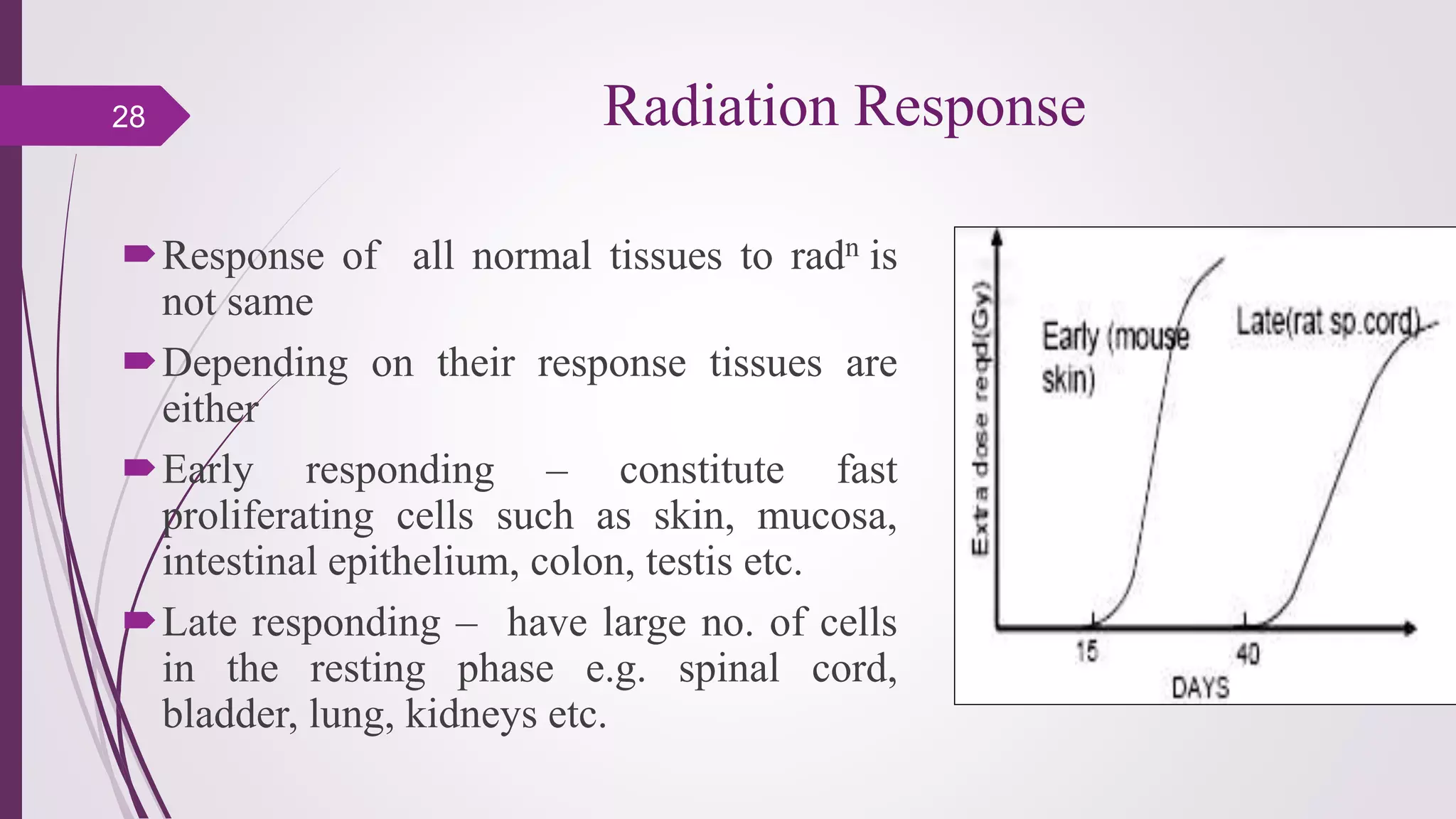
Fractionation in radiotherapy refers to dividing the total radiation dose into smaller doses given over multiple treatment sessions. This allows healthy cells to repair sublethal damage between fractions while maximizing cancer cell kill through mechanisms like redistribution and reoxygenation. The "5 R's" of radiobiology explain fractionation: repair of sublethal damage in normal cells; redistribution of tumor cells to sensitive phases; reoxygenation of hypoxic tumor cells; repopulation of tumor cells during prolonged treatment; and intrinsic radiosensitivity differences between cell types. Fractionation schedules are tailored based on these factors to improve the therapeutic ratio for different cancers and patients.