Downloaded 294 times


![VASCULAR INVASION
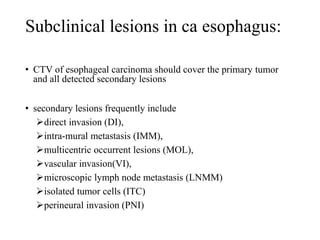
• defined as the infiltration of tumor cells into lymph and blood vessels, as
well as tumor embolus formation.
• The incidence of VI in early-stage ESCC was 13.89% (15/108) [14] and
39.1% (143/366) in advanced disease [15].
• The incidence of VI in esophageal adenocarcinoma was 49.9% (229/459)
[16].
• All of these studies demonstrated that VI is an important prognostic factor;
however, none of these studies assessed the distance of VI sites from the
primary tumor
14. Amano T et al. Subepithelial extension of squamouscell carcinoma in the esophagus: histopathological study using
D2-40 immunostaining for 108 superficial carcinomas. Pathol Int. 2007;57:759-64.
15. Brücher BL et al. Lymphatic vessel invasion is an independentprognostic factor in patients with a primary resected
tumor withesophageal squamous cell carcinoma. Cancer. 2001;92:2228-33.
16. von Rahden BH, et al. Lymphatic vessel invasion as aprognostic factor in patients with primary resected
adenocarcinomas of theesophagogastric junction. J Clin Oncol. 2005;23:874-9.
17. Koenig AM, et al. Strong impact of micrometastatictumor cell load in patients with esophageal carcinoma. Ann
Surg Oncol.2009;16:454-62.](https://image.slidesharecdn.com/radiotherapyincaesophagus-190622055742/85/Radiotherapy-in-ca-esophagus-15-320.jpg)

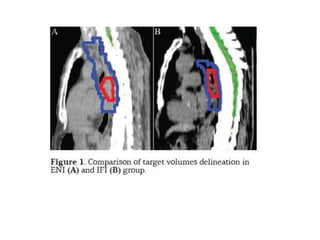
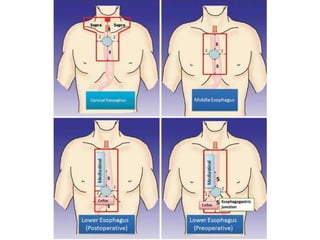
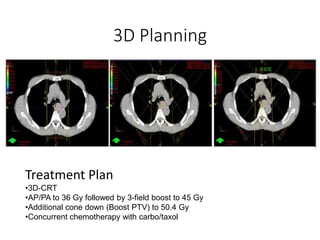

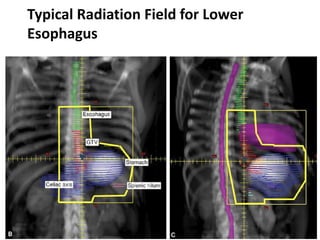
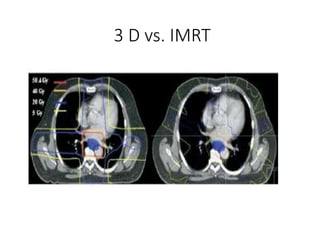
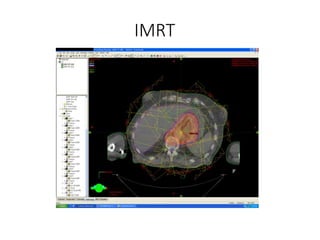
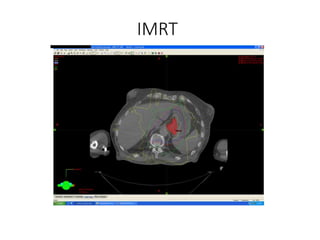
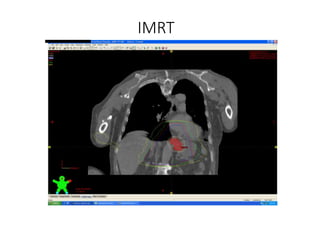

1) The document discusses various radiation techniques for treating cancer of the esophagus including 2D, 3D conformal radiation therapy, IMRT, and IGRT. 2) It covers topics like target volume delineation, field design considerations for different esophageal subsites, and evolution from 2D to 3D treatment planning. 3) While there is no consensus, most contemporary trials use margins of 3-5cm cranially and caudally on the gross tumor with approximately a 2cm radial margin.








![Arc therapy [autosaved] [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/arctherapyautosavedautosaved-150423125828-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)




































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









