Download to read offline
![Pyramidal system
Keshav Kumar Panwar[Group 9]
2nd year 1st Semester
Kursk State Medical University](https://image.slidesharecdn.com/pyramidalsystem-221213201348-950ec3dc/85/Pyramidal-system-Keshav-Kumar-Panwar-pptx-1-320.jpg)



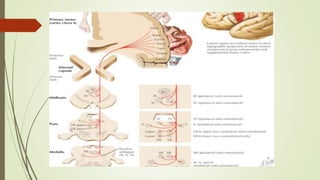


The pyramidal system consists of two main tracts - the corticospinal tract and the corticobulbar tract. These tracts originate from the cerebral cortex and carry motor signals to the spinal cord and brainstem. Nerve fibers in these tracts terminate on motor neurons and interneurons in the spinal cord and brainstem, controlling voluntary muscle movements and influencing reflexes. Damage to the pyramidal tracts can result in symptoms like spasticity and abnormal reflexes due to disruption of signals controlling motor functions.























































































