Download as PDF, PPTX

























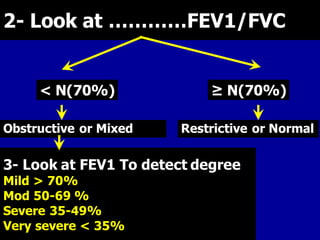

















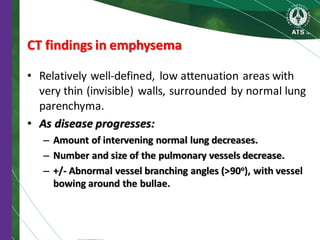













































This document provides information on diagnosing and differentially diagnosing COPD, including: - Key indicators that should prompt consideration of a COPD diagnosis including dyspnea, chronic cough, sputum production, and risk factor exposure. Spirometry is required to confirm COPD. - Spirometry is the basic investigation needed to diagnose COPD. It assesses airflow limitation through FEV1/FVC ratio and severity through FEV1 levels. Reversibility testing can help differentiate COPD from asthma. - Additional optional investigations that may be used include imaging like chest X-rays and CT scans to identify emphysema and airway abnormalities, lung volume measurements, diffusing capacity tests, and

















![Copd And The Gold Guidelines 02 21 2005[2]](https://cdn.slidesharecdn.com/ss_thumbnails/copd-and-the-gold-guidelines-022120052-1233826160411176-2-thumbnail.jpg?width=640&height=640&fit=bounds)











































































