Download to read offline
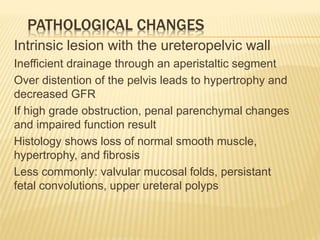
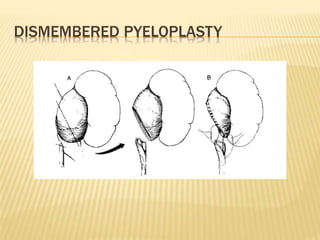


UPJ obstruction is a common cause of urinary tract obstruction in children, primarily identified antenatally, and occurs more frequently in males. Diagnosis typically involves ultrasound, with significant variability in interpretation and outcomes; indications for surgical intervention include symptoms and impaired renal function. Surgical options range from open pyeloplasty to laparoscopic techniques, with ongoing monitoring of obstructed kidneys to determine the necessity for intervention.




















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


