Download to read offline

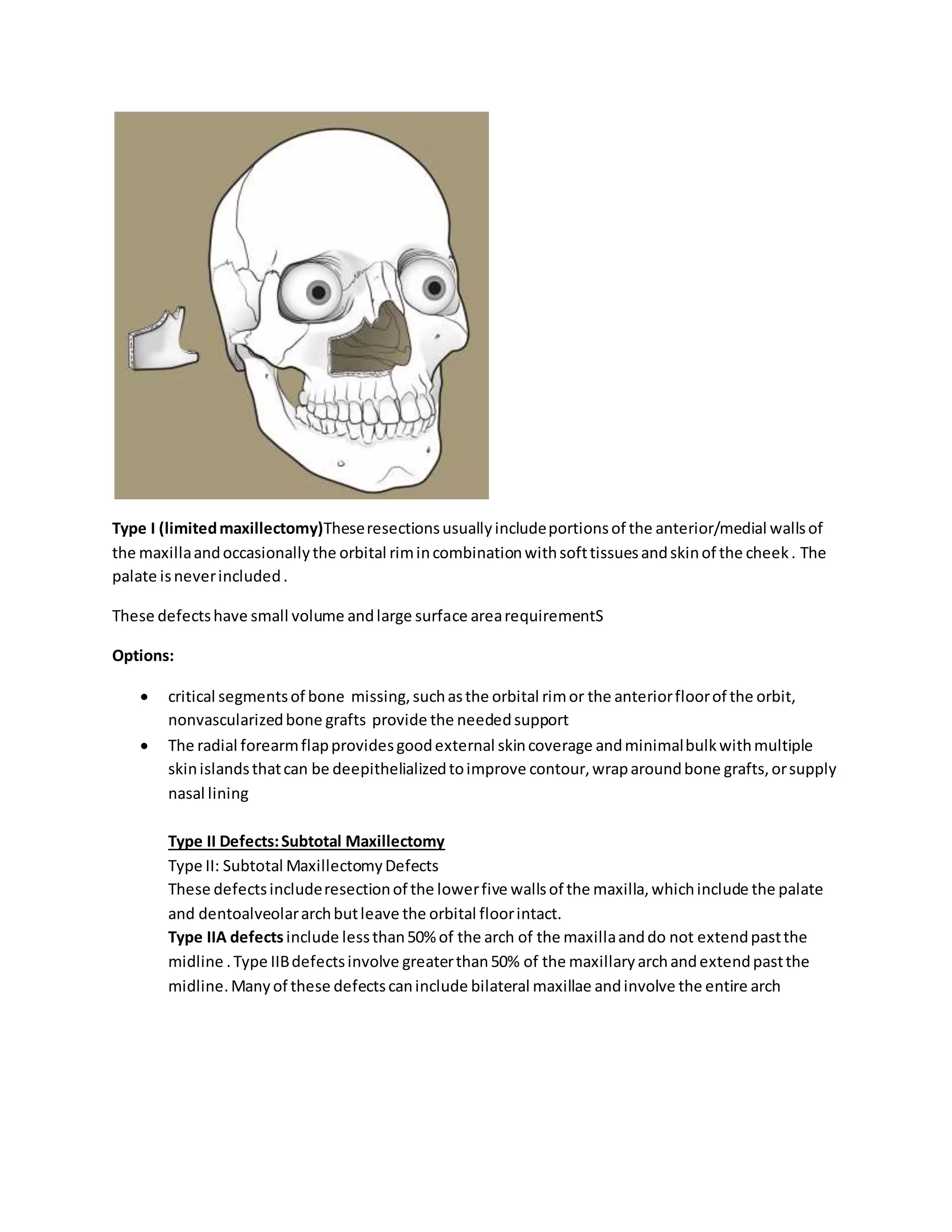
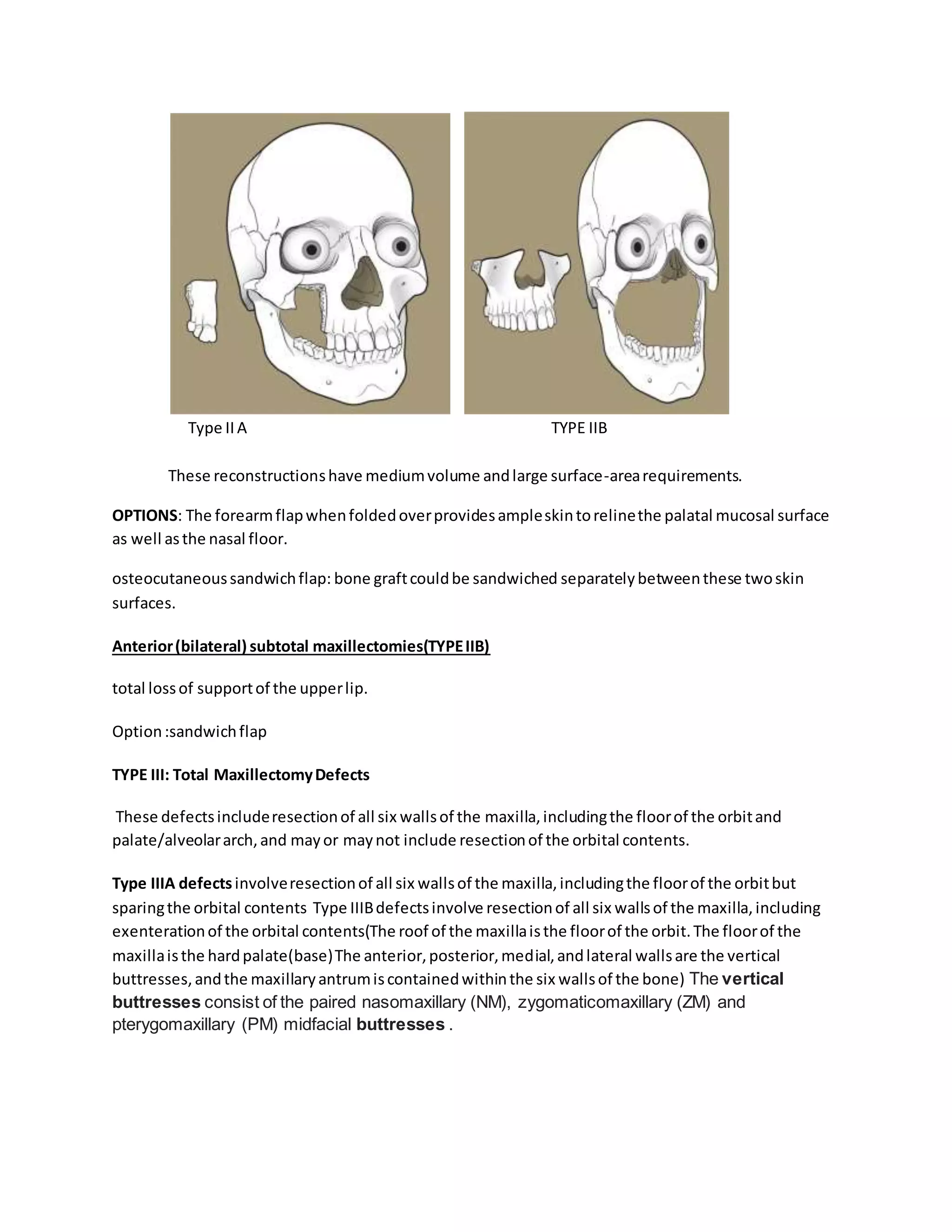

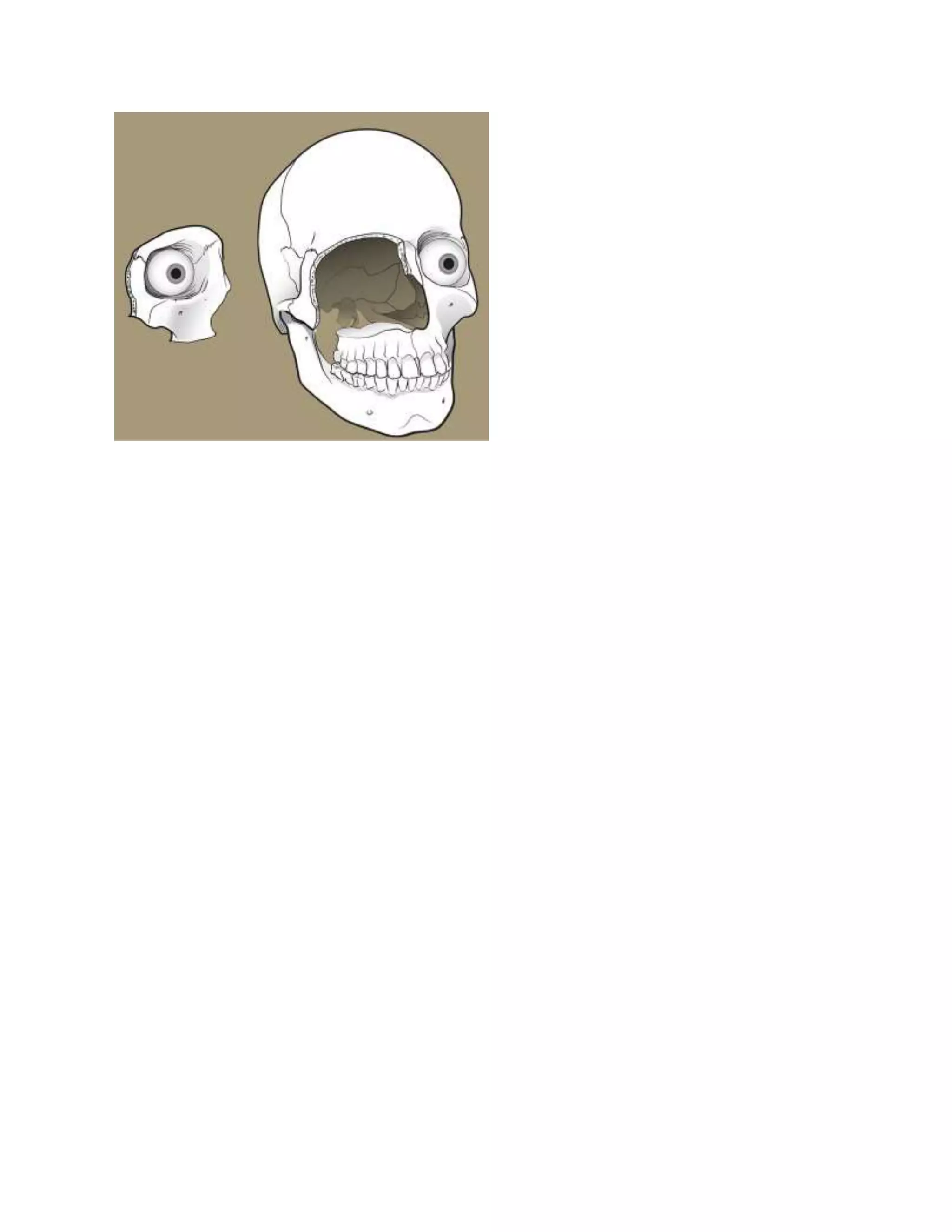

This document classifies and describes different types of maxillectomy defects based on the extent of resection. It discusses four main types of defects: Type I defects involve limited resection of one or two maxillary walls excluding the palate. Type II defects resect the maxillary arch, palate, and anterior/lateral walls while preserving the orbital floor. Type III defects resect all six maxillary walls, with Type IIIa preserving the orbit and IIIb including orbital exenteration. Type IV defects resect the upper five maxillary walls and orbital contents. The document outlines reconstruction options for each defect type based on the volume and surface area requirements. Non-vascularized bone grafts or forearm























































































