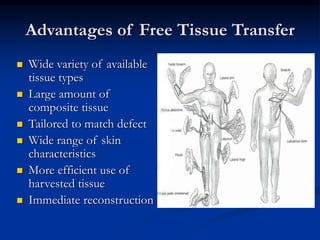
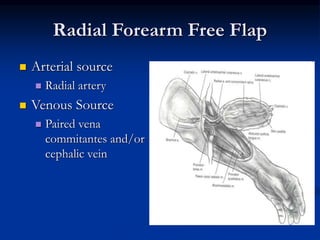
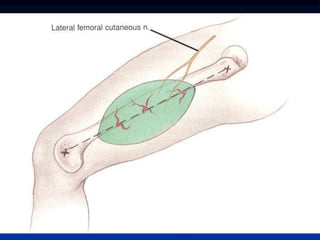
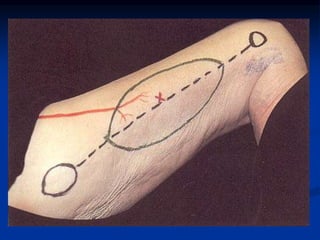
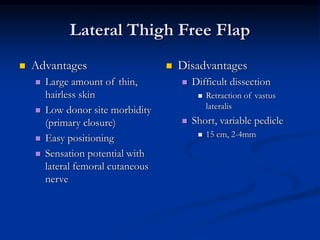
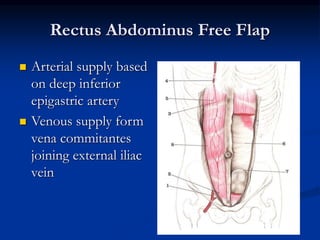
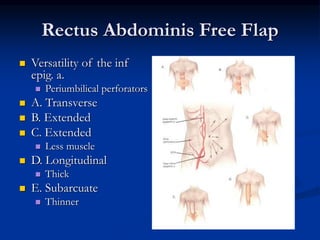
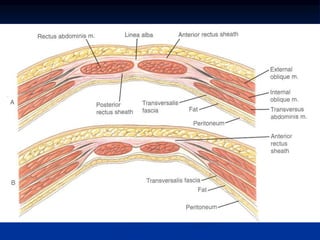
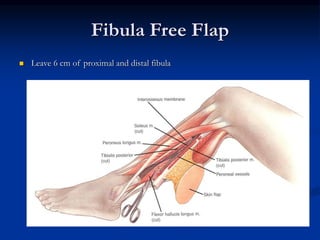
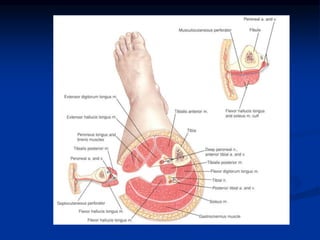
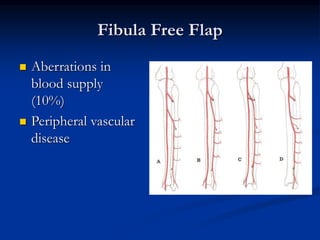
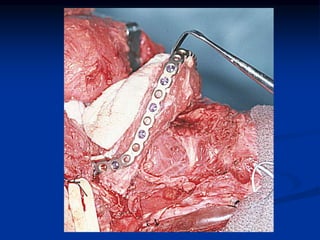
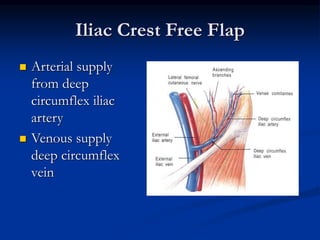
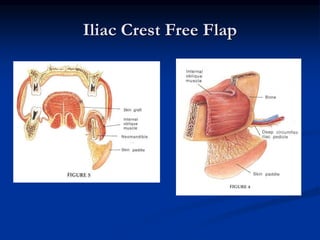
This document provides an overview of free flap reconstruction techniques for head and neck defects. It discusses the history and evolution of free flaps, describes various flap types including fasciocutaneous, musculocutaneous, and composite flaps, and covers considerations for preoperative planning and intraoperative management. Key free flap options described include the radial forearm flap, lateral thigh flap, rectus abdominis flap, fibula flap, and jejunum flap. The document emphasizes that free flaps allow for tailored reconstruction with a variety of tissue types to match specific defect needs.