Downloaded 25 times



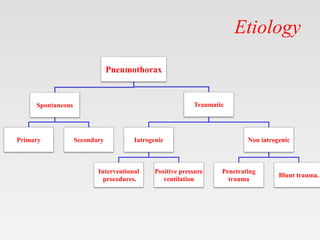







This document provides tips and instructions for using a PowerPoint presentation on pneumothorax. The presentation contains blank slides where students can provide their knowledge on topics before seeing the slides with information. Using this active learning technique over three revisions will make for an effective self-study or teaching session. The presentation covers definitions, causes, mechanisms, clinical features, diagnosis and management of pneumothorax. QR codes and links are also provided to access the full presentation on mobile devices or download additional teaching materials.























































































