Downloaded 26 times

![Convex visceral pleuralChest wall
By Mikael Häggström [CC0], from Wikimedia Commons](https://image.slidesharecdn.com/pneumothorax-190625202505/85/Pneumothorax-13-320.jpg)
![By Karthik Easvur [CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0)], from Wikimedia Commons](https://image.slidesharecdn.com/pneumothorax-190625202505/85/Pneumothorax-15-320.jpg)
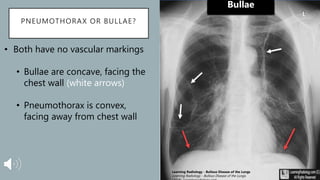
![Convex
Concave
By Mikael Häggström [CC0], from Wikimedia Commons
Learning Radiology - Bullous Disease of the Lungs
Learning Radiology - Bullous Disease of the Lungs.
(2018). Learningradiology.com.
Bullous Disease Pneumothorax](https://image.slidesharecdn.com/pneumothorax-190625202505/85/Pneumothorax-17-320.jpg)
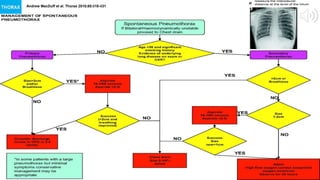

1. The document discusses spontaneous pneumothorax, focusing on diagnosis and management. 2. Key points covered include risk factors for primary and secondary spontaneous pneumothorax, clinical evaluation, imaging studies, and criteria for determining appropriate treatment including observation, needle aspiration, chest tube insertion, or referral to cardiothoracic surgery. 3. Management decisions are based on whether the pneumothorax is primary or secondary, the patient's symptoms, and the size of the pneumothorax.



































































