This document provides an overview of pneumothorax. It begins by defining pneumothorax as air in the pleural space between the lung and chest wall. The pathophysiology section explains how a pneumothorax occurs when air leaks into the pleural space, eliminating the normal negative pressure. This can impair breathing and circulation.
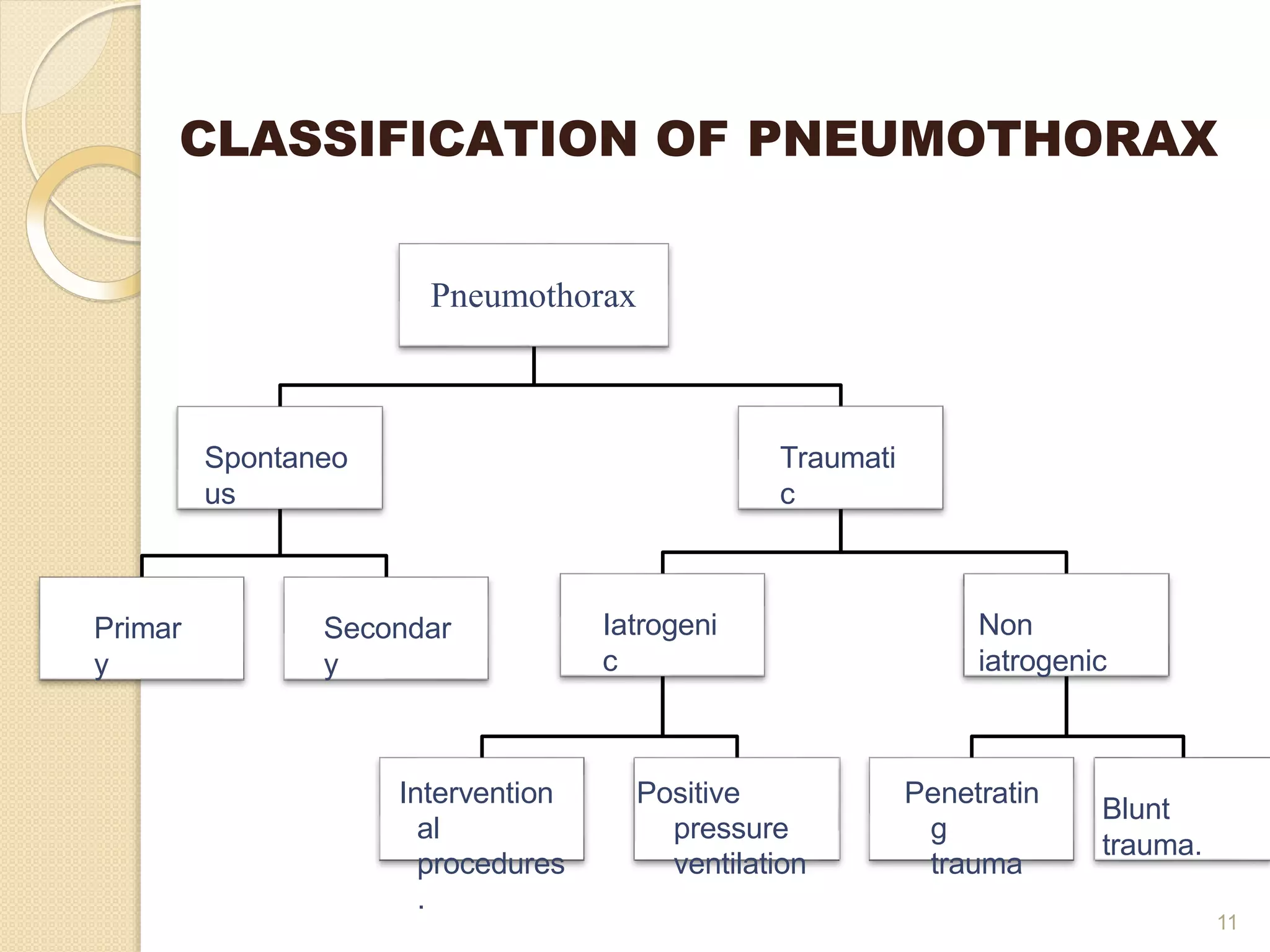
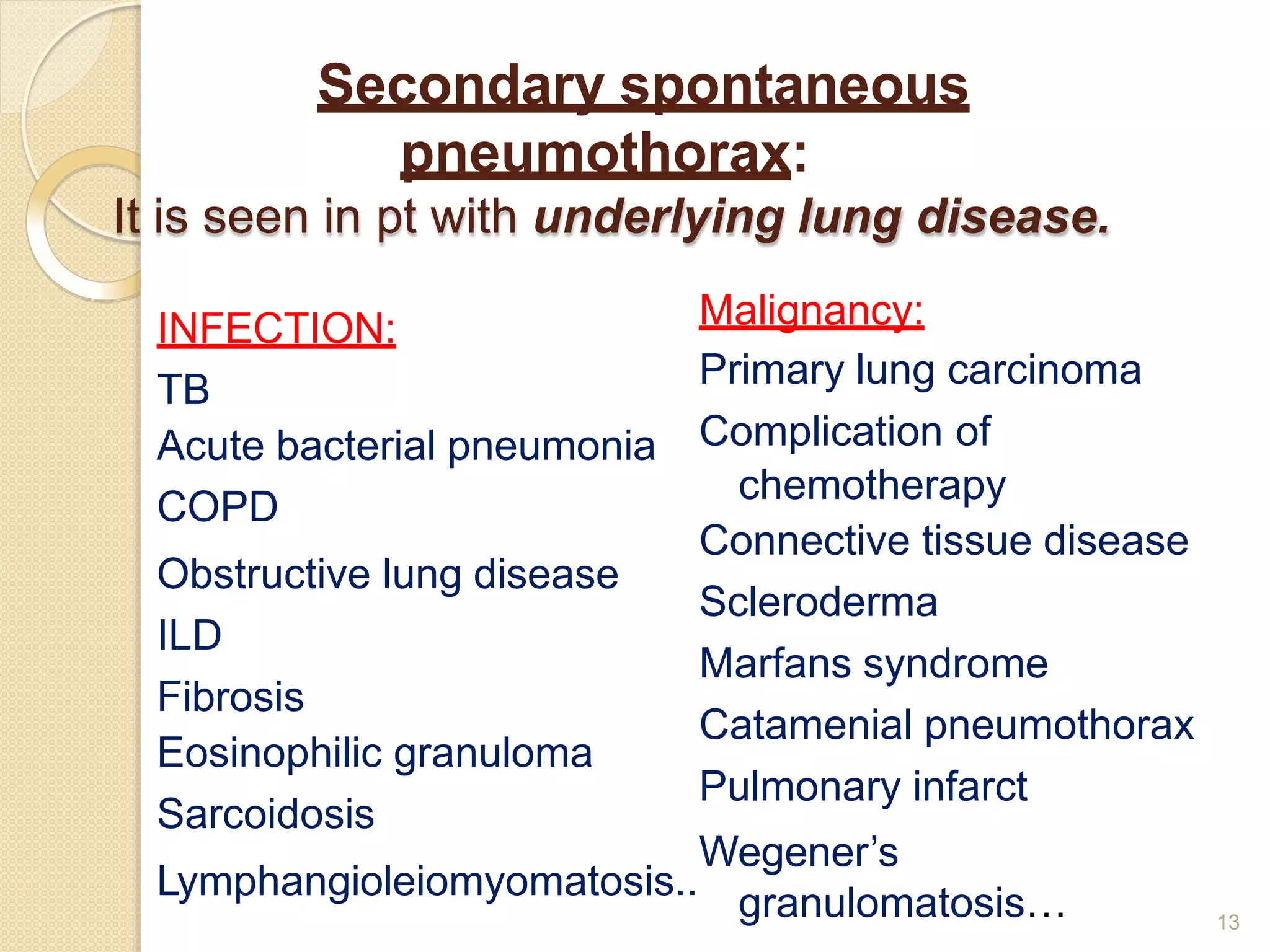
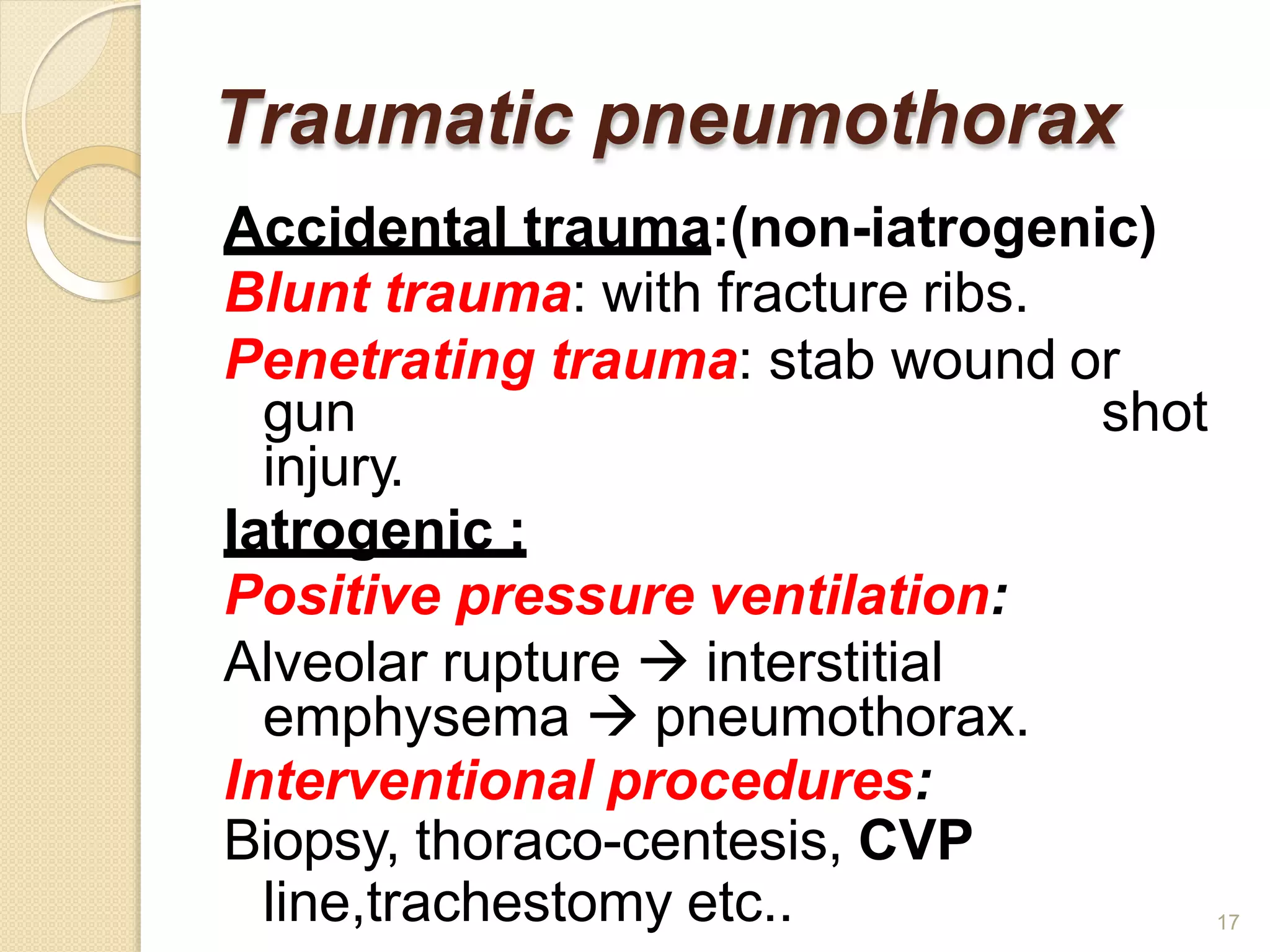
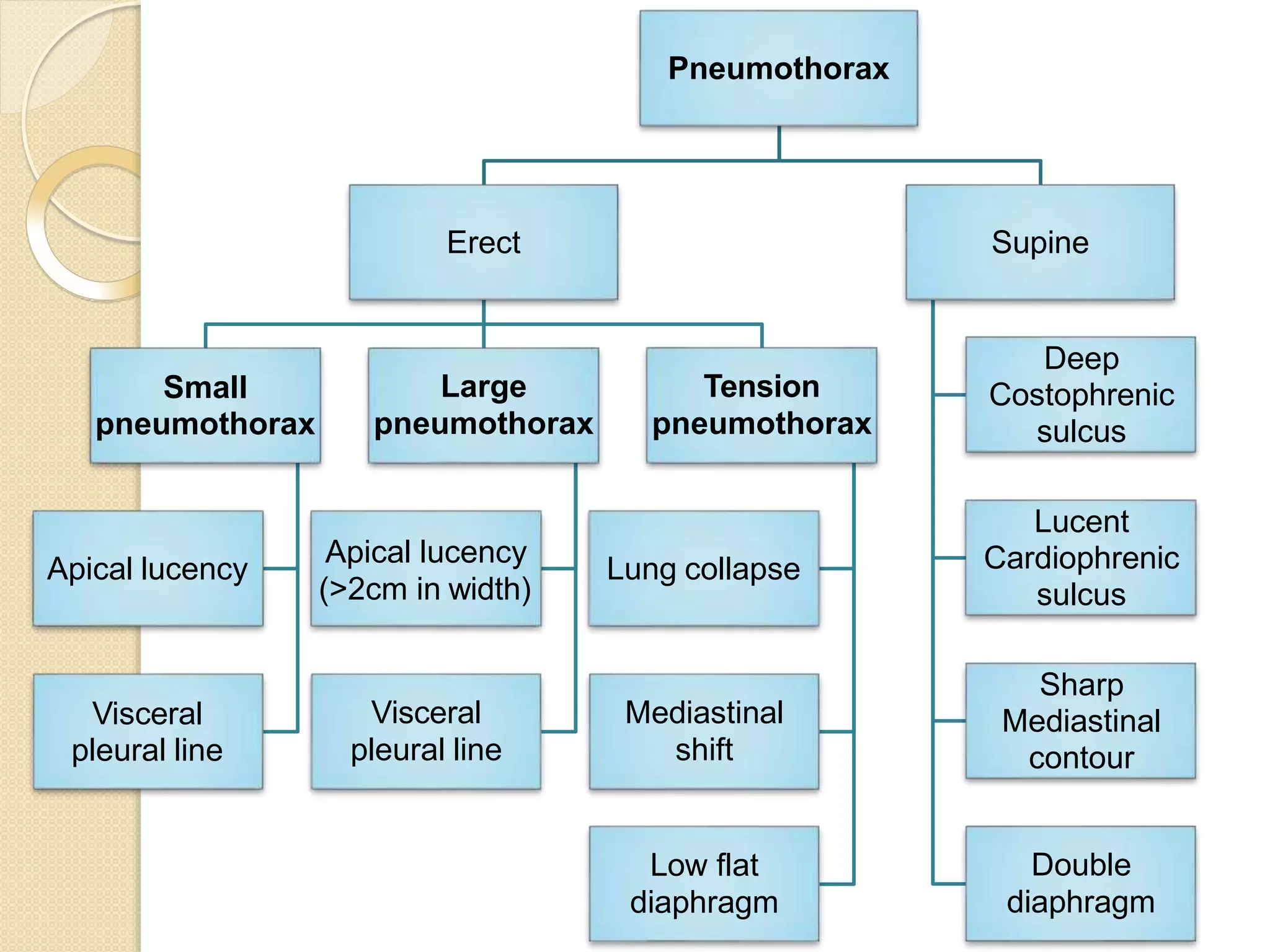
The document then classifies pneumothoraces as primary spontaneous, secondary spontaneous, or traumatic. Clinical features include dyspnea and chest pain. Diagnosis involves chest x-ray or CT scan to evaluate lung collapse and estimate size. Treatment depends on pneumothorax type and size but may include observation, oxygen therapy, needle aspiration, chest tube drainage, chemical pleuro