Downloaded 1,204 times




















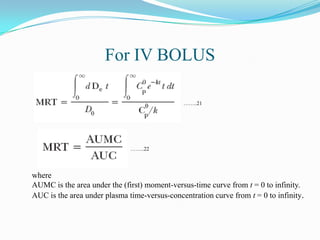
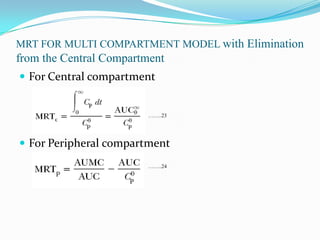



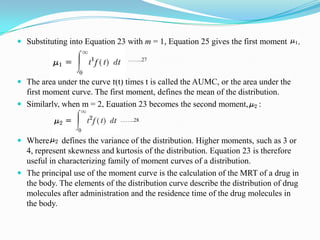



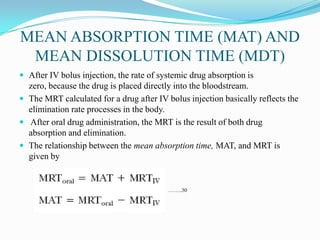





This document discusses physiological pharmacokinetic models, which describe drug movement and disposition in the body based on organ blood flow and organ spaces penetrated by the drug. It presents different types of models, including blood flow-limited models, models incorporating drug binding, and membrane-limited models. It discusses key concepts like mean residence time, mean absorption time, and mean dissolution time. Physiological pharmacokinetic models provide a more exact description of drug concentrations over time compared to non-physiological models.



































































