Downloaded 1,243 times
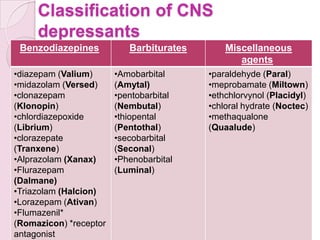
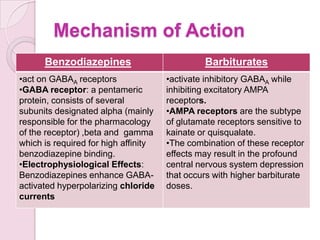
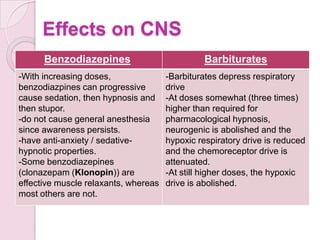
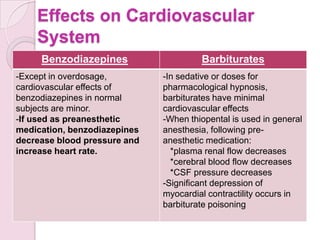
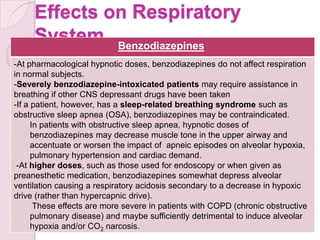
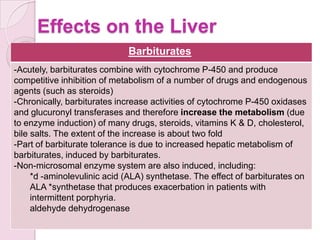
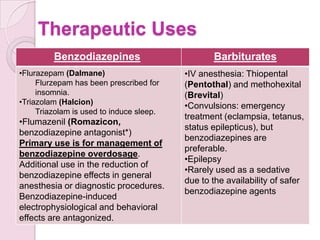

This document discusses drugs that act on the central nervous system (CNS), specifically sedative-hypnotic drugs. It covers the classification of CNS depressants like benzodiazepines and barbiturates. It describes their mechanisms of action, effects on the CNS, cardiovascular system, respiratory system, and liver. It also discusses their therapeutic uses, adverse effects, dependence and abuse potential, as well as management of overdoses.







































![4._Sedative_hypnotics[1].pptx pharmacy students](https://cdn.slidesharecdn.com/ss_thumbnails/4-251117163021-acac7ad2-thumbnail.jpg?width=640&height=640&fit=bounds)

























![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











