Downloaded 75 times




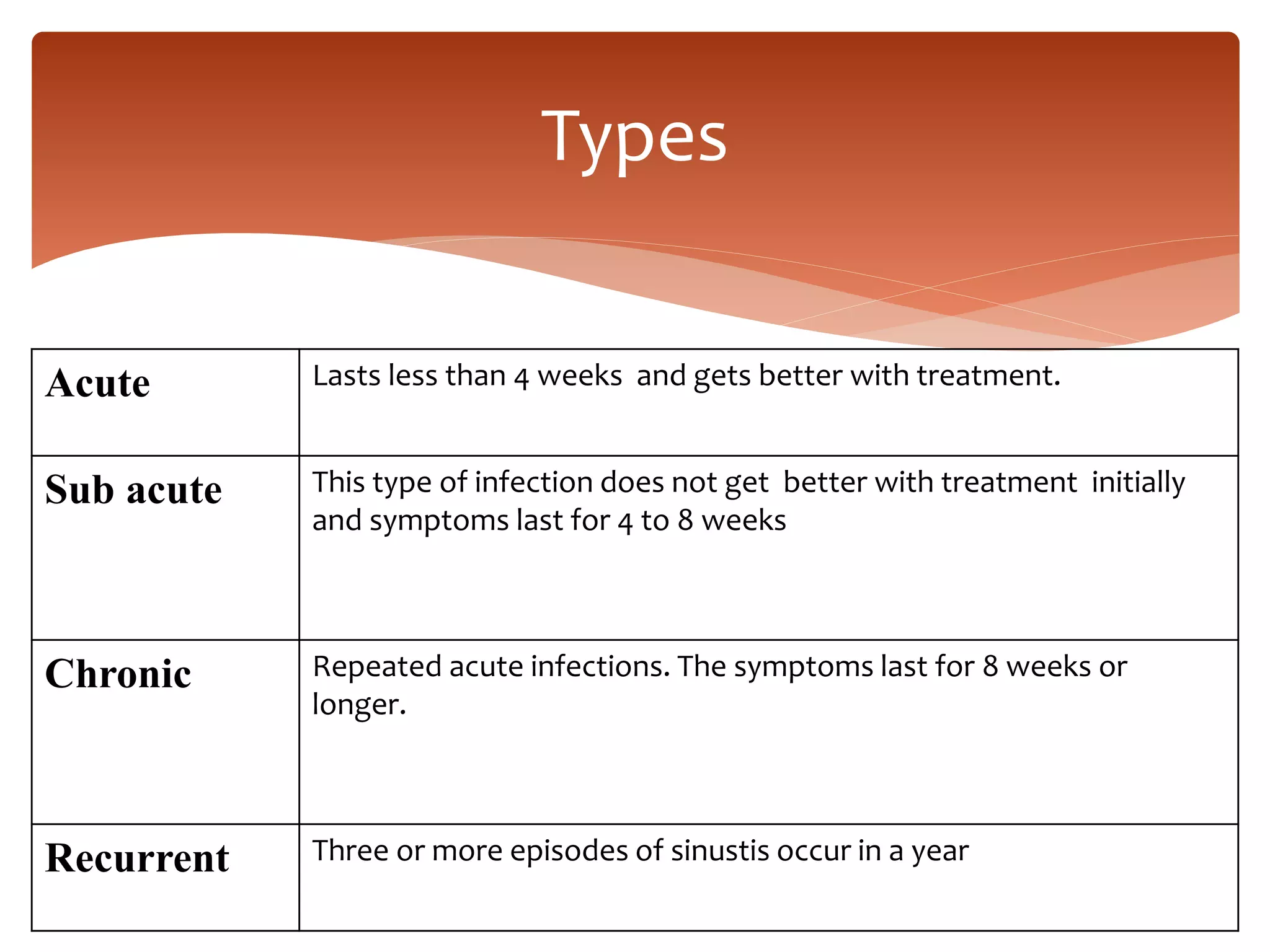











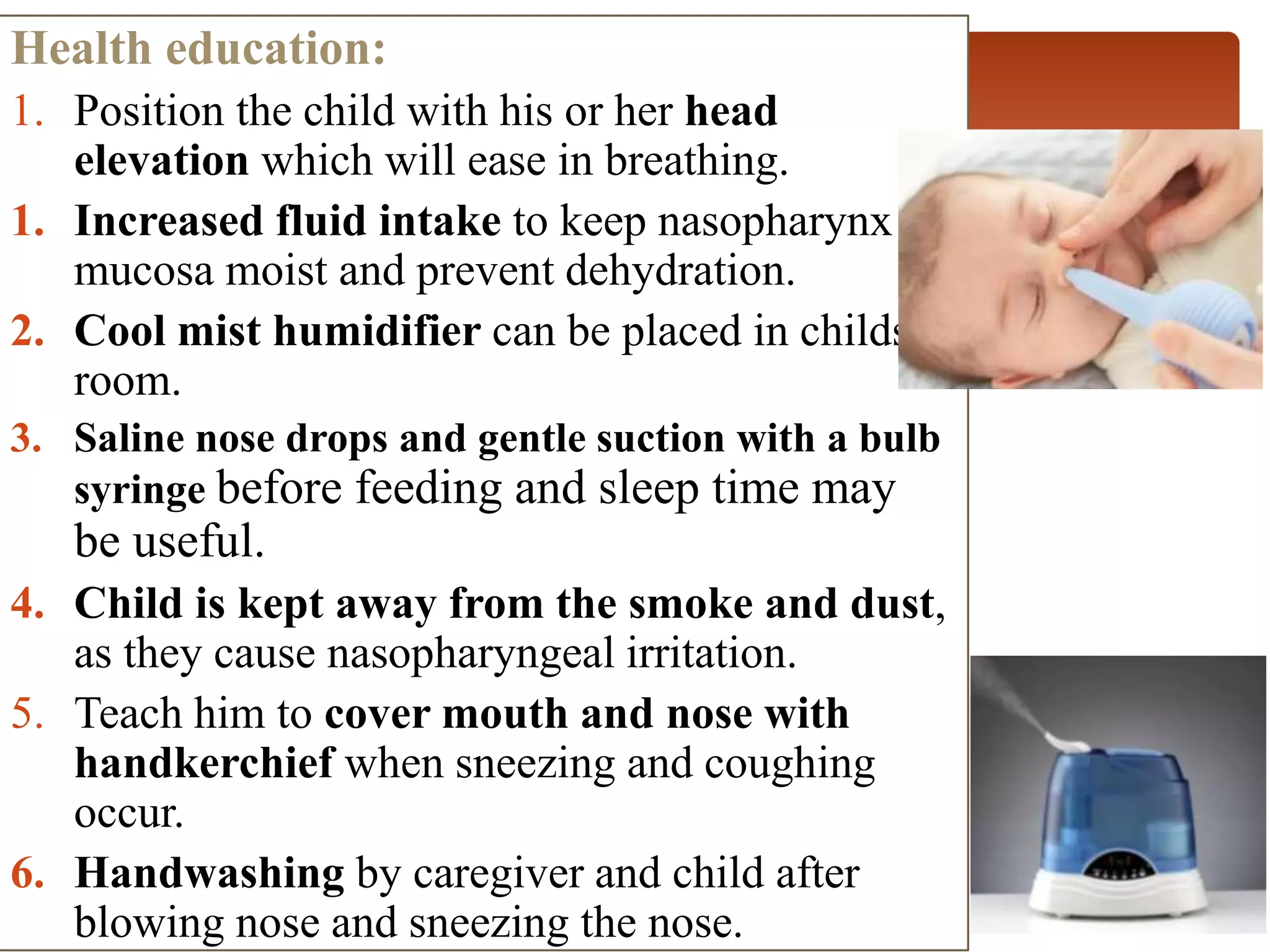


























The document provides a comprehensive overview of upper respiratory tract infections, focusing on sinusitis, nasopharyngitis, stridor, pharyngitis, tonsillitis, and croup, including definitions, causes, symptoms, diagnostic approaches, and treatment methods. It details the necessary medical and nursing management for each condition, emphasizing symptom relief, hydration, and possible surgical interventions. The document also highlights the importance of health education for caregivers and parents in managing these conditions.