Downloaded 2,439 times

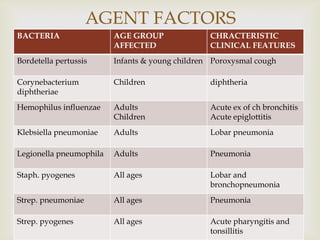
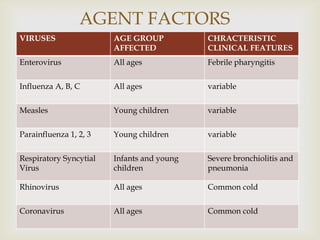




Acute respiratory infections (ARI) are responsible for 20% of childhood deaths under 5 years of age, with pneumonia accounting for 90% of ARI mortality. Children under 2 years old, malnourished children, children with HIV, and those with poor access to healthcare or poorly educated parents are most at risk. ARIs are a common cause of outpatient visits (20-60%) and admissions (12-45%) in children. Common respiratory infections affecting children include the common cold, acute epiglottitis, croup, ear infections, tonsillitis, sinusitis, and pneumonia. Bacteria and viruses can cause ARIs, with symptoms and severity depending on the specific infectious agent.














































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)








