This document discusses the management of upper respiratory tract infections. It begins by outlining the objectives and topics to be covered, including viral rhinitis, acute and chronic pharyngitis and tonsillitis, epistaxis, and cancer of the larynx. For each condition, it describes the etiology, clinical manifestations, diagnostic findings, medical management, and nursing management. Surgical procedures for cancer of the larynx and postoperative care are also outlined. The document provides a comprehensive overview of assessing and treating various upper respiratory infections and conditions.
oxygen is very very important for the human being. so i tried here to provide best content from the books and easy way to understand, if you like this slide comment it.
THIS presentation EXPLAINS biomedical waste management IN EASY WAY
Important links- NOTES- https://mynursingstudents.blogspot.com/
youtube channel
https://www.youtube.com/c/MYSTUDENTSU...
CHANEL PLAYLIST-
ANATOMY AND PHYSIOLOGY-https://www.youtube.com/playlist?list...
COMMUNITY HEALTH NURSING- https://www.youtube.com/playlist?list...
CHILD HEALTH NURSING- https://www.youtube.com/playlist?list...
FIRST AID- https://www.youtube.com/playlist?list...
HCM- https://www.youtube.com/playlist?list...
FUNDAMENTALS OF NURSING- https://www.youtube.com/playlist?list...
COMMUNICABLE DISEASES- https://www.youtube.com/playlist?list...
ENVIRONMENTAL HEALTH- https://www.youtube.com/playlist?list...
MSN- https://www.youtube.com/playlist?list...
HINDI ONLY- https://www.youtube.com/playlist?list...
ENGLISH ONLY- https://www.youtube.com/playlist?list...
facebook profile- https://www.facebook.com/suresh.kr.lrhs/
FACEBOOK PAGE- https://www.facebook.com/My-Student-S...
facebook group NURSING NOTES- https://www.facebook.com/groups/24139...
FOR MAKING EASY NOTES YOU CAN ALSO VISIT MY BLOG –
BLOGGER- https://mynursingstudents.blogspot.com/
Instagram- https://www.instagram.com/mystudentsu...
Twitter- https://twitter.com/student_system?s=08
#VITAMIN_A,#FUNCTIONS,#SOURCE, #DEFICIENCY,#DISEASE,#NIGHTBLINDNESS#XEROPHTHALMIA,#BITOTSPOT,#CORNEALXEROSIS, #CONJUNCIVALXEROSIS, YELLOWFRUITS,#MYSTUDENTSUPPORTSYSTEM, #rashes,#nursingclasses, #communityhealthnursing,#ANM, #GNM, #BSCNURING,#NURSINGSTUDENTS, #WHO,#NURSINGINSTITUTION,#COLLEGEOFNURSING,#nursingofficer,#COMMUNITYHEALTHOFFICER
CASE STUDY ON -UTI(Urinary Tract Infection)Pranab Mandal
Case study on UTI# case presentation for UTI# case presentation for UTI# case study Urinary tract Infection # Case study on UTI # case presentation UTI # case study UTI # Case study UTI # case study on UTI # case presentation on UTI # case presentation nephrotic syndrome # and 2k24 january # Nursing # Xase presentation on UTI
oxygen is very very important for the human being. so i tried here to provide best content from the books and easy way to understand, if you like this slide comment it.
THIS presentation EXPLAINS biomedical waste management IN EASY WAY
Important links- NOTES- https://mynursingstudents.blogspot.com/
youtube channel
https://www.youtube.com/c/MYSTUDENTSU...
CHANEL PLAYLIST-
ANATOMY AND PHYSIOLOGY-https://www.youtube.com/playlist?list...
COMMUNITY HEALTH NURSING- https://www.youtube.com/playlist?list...
CHILD HEALTH NURSING- https://www.youtube.com/playlist?list...
FIRST AID- https://www.youtube.com/playlist?list...
HCM- https://www.youtube.com/playlist?list...
FUNDAMENTALS OF NURSING- https://www.youtube.com/playlist?list...
COMMUNICABLE DISEASES- https://www.youtube.com/playlist?list...
ENVIRONMENTAL HEALTH- https://www.youtube.com/playlist?list...
MSN- https://www.youtube.com/playlist?list...
HINDI ONLY- https://www.youtube.com/playlist?list...
ENGLISH ONLY- https://www.youtube.com/playlist?list...
facebook profile- https://www.facebook.com/suresh.kr.lrhs/
FACEBOOK PAGE- https://www.facebook.com/My-Student-S...
facebook group NURSING NOTES- https://www.facebook.com/groups/24139...
FOR MAKING EASY NOTES YOU CAN ALSO VISIT MY BLOG –
BLOGGER- https://mynursingstudents.blogspot.com/
Instagram- https://www.instagram.com/mystudentsu...
Twitter- https://twitter.com/student_system?s=08
#VITAMIN_A,#FUNCTIONS,#SOURCE, #DEFICIENCY,#DISEASE,#NIGHTBLINDNESS#XEROPHTHALMIA,#BITOTSPOT,#CORNEALXEROSIS, #CONJUNCIVALXEROSIS, YELLOWFRUITS,#MYSTUDENTSUPPORTSYSTEM, #rashes,#nursingclasses, #communityhealthnursing,#ANM, #GNM, #BSCNURING,#NURSINGSTUDENTS, #WHO,#NURSINGINSTITUTION,#COLLEGEOFNURSING,#nursingofficer,#COMMUNITYHEALTHOFFICER
CASE STUDY ON -UTI(Urinary Tract Infection)Pranab Mandal
Case study on UTI# case presentation for UTI# case presentation for UTI# case study Urinary tract Infection # Case study on UTI # case presentation UTI # case study UTI # Case study UTI # case study on UTI # case presentation on UTI # case presentation nephrotic syndrome # and 2k24 january # Nursing # Xase presentation on UTI
Tepid Sponge Bath lecture and procedure for First Year Level Nursing students during their Return Demonstration. This is taken from a procedure manual good for both students and instructor.
Urinary catheterisation is a procedure used to drain the bladder and collect urine, through a flexible tube called a catheter. Urinary catheters are usually inserted by doctors or nurses in hospital or the community
role of nurse in medical surgical setting.pptxDrsuhelKhan2
this slide upload for increase the knowledge of nursing student's, and by the help of this students learn about the various roles and responsibilities of nurse in Medical Surgical Setting.
Tepid Sponge Bath lecture and procedure for First Year Level Nursing students during their Return Demonstration. This is taken from a procedure manual good for both students and instructor.
Urinary catheterisation is a procedure used to drain the bladder and collect urine, through a flexible tube called a catheter. Urinary catheters are usually inserted by doctors or nurses in hospital or the community
role of nurse in medical surgical setting.pptxDrsuhelKhan2
this slide upload for increase the knowledge of nursing student's, and by the help of this students learn about the various roles and responsibilities of nurse in Medical Surgical Setting.
UPPER RESIRATORY TRACT INFECTIONS IN CHILDREN , ACUE PHARYGITIS , COMMON COLD , ACUTE SINUSITIS , ACUTE OTITIS MEDIA , APPROACH TO PATIENT WITH URTI , MANAGEMENT OF URTI IN CHILDREN
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
ARTIFICIAL INTELLIGENCE IN HEALTHCARE.pdfAnujkumaranit
Artificial intelligence (AI) refers to the simulation of human intelligence processes by machines, especially computer systems. It encompasses tasks such as learning, reasoning, problem-solving, perception, and language understanding. AI technologies are revolutionizing various fields, from healthcare to finance, by enabling machines to perform tasks that typically require human intelligence.
- Video recording of this lecture in English language: https://youtu.be/lK81BzxMqdo
- Video recording of this lecture in Arabic language: https://youtu.be/Ve4P0COk9OI
- Link to download the book free: https://nephrotube.blogspot.com/p/nephrotube-nephrology-books.html
- Link to NephroTube website: www.NephroTube.com
- Link to NephroTube social media accounts: https://nephrotube.blogspot.com/p/join-nephrotube-on-social-media.html
HOT NEW PRODUCT! BIG SALES FAST SHIPPING NOW FROM CHINA!! EU KU DB BK substit...GL Anaacs
Contact us if you are interested:
Email / Skype : kefaya1771@gmail.com
Threema: PXHY5PDH
New BATCH Ku !!! MUCH IN DEMAND FAST SALE EVERY BATCH HAPPY GOOD EFFECT BIG BATCH !
Contact me on Threema or skype to start big business!!
Hot-sale products:
NEW HOT EUTYLONE WHITE CRYSTAL!!
5cl-adba precursor (semi finished )
5cl-adba raw materials
ADBB precursor (semi finished )
ADBB raw materials
APVP powder
5fadb/4f-adb
Jwh018 / Jwh210
Eutylone crystal
Protonitazene (hydrochloride) CAS: 119276-01-6
Flubrotizolam CAS: 57801-95-3
Metonitazene CAS: 14680-51-4
Payment terms: Western Union,MoneyGram,Bitcoin or USDT.
Deliver Time: Usually 7-15days
Shipping method: FedEx, TNT, DHL,UPS etc.Our deliveries are 100% safe, fast, reliable and discreet.
Samples will be sent for your evaluation!If you are interested in, please contact me, let's talk details.
We specializes in exporting high quality Research chemical, medical intermediate, Pharmaceutical chemicals and so on. Products are exported to USA, Canada, France, Korea, Japan,Russia, Southeast Asia and other countries.
Ethanol (CH3CH2OH), or beverage alcohol, is a two-carbon alcohol
that is rapidly distributed in the body and brain. Ethanol alters many
neurochemical systems and has rewarding and addictive properties. It
is the oldest recreational drug and likely contributes to more morbidity,
mortality, and public health costs than all illicit drugs combined. The
5th edition of the Diagnostic and Statistical Manual of Mental Disorders
(DSM-5) integrates alcohol abuse and alcohol dependence into a single
disorder called alcohol use disorder (AUD), with mild, moderate,
and severe subclassifications (American Psychiatric Association, 2013).
In the DSM-5, all types of substance abuse and dependence have been
combined into a single substance use disorder (SUD) on a continuum
from mild to severe. A diagnosis of AUD requires that at least two of
the 11 DSM-5 behaviors be present within a 12-month period (mild
AUD: 2–3 criteria; moderate AUD: 4–5 criteria; severe AUD: 6–11 criteria).
The four main behavioral effects of AUD are impaired control over
drinking, negative social consequences, risky use, and altered physiological
effects (tolerance, withdrawal). This chapter presents an overview
of the prevalence and harmful consequences of AUD in the U.S.,
the systemic nature of the disease, neurocircuitry and stages of AUD,
comorbidities, fetal alcohol spectrum disorders, genetic risk factors, and
pharmacotherapies for AUD.
These lecture slides, by Dr Sidra Arshad, offer a quick overview of physiological basis of a normal electrocardiogram.
Learning objectives:
1. Define an electrocardiogram (ECG) and electrocardiography
2. Describe how dipoles generated by the heart produce the waveforms of the ECG
3. Describe the components of a normal electrocardiogram of a typical bipolar leads (limb II)
4. Differentiate between intervals and segments
5. Enlist some common indications for obtaining an ECG
Study Resources:
1. Chapter 11, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 9, Human Physiology - From Cells to Systems, Lauralee Sherwood, 9th edition
3. Chapter 29, Ganong’s Review of Medical Physiology, 26th edition
4. Electrocardiogram, StatPearls - https://www.ncbi.nlm.nih.gov/books/NBK549803/
5. ECG in Medical Practice by ABM Abdullah, 4th edition
6. ECG Basics, http://www.nataliescasebook.com/tag/e-c-g-basics
Prix Galien International 2024 Forum ProgramLevi Shapiro
June 20, 2024, Prix Galien International and Jerusalem Ethics Forum in ROME. Detailed agenda including panels:
- ADVANCES IN CARDIOLOGY: A NEW PARADIGM IS COMING
- WOMEN’S HEALTH: FERTILITY PRESERVATION
- WHAT’S NEW IN THE TREATMENT OF INFECTIOUS,
ONCOLOGICAL AND INFLAMMATORY SKIN DISEASES?
- ARTIFICIAL INTELLIGENCE AND ETHICS
- GENE THERAPY
- BEYOND BORDERS: GLOBAL INITIATIVES FOR DEMOCRATIZING LIFE SCIENCE TECHNOLOGIES AND PROMOTING ACCESS TO HEALTHCARE
- ETHICAL CHALLENGES IN LIFE SCIENCES
- Prix Galien International Awards Ceremony
263778731218 Abortion Clinic /Pills In Harare ,sisternakatoto
263778731218 Abortion Clinic /Pills In Harare ,ABORTION WOMEN’S CLINIC +27730423979 IN women clinic we believe that every woman should be able to make choices in her pregnancy. Our job is to provide compassionate care, safety,affordable and confidential services. That’s why we have won the trust from all generations of women all over the world. we use non surgical method(Abortion pills) to terminate…Dr.LISA +27730423979women Clinic is committed to providing the highest quality of obstetrical and gynecological care to women of all ages. Our dedicated staff aim to treat each patient and her health concerns with compassion and respect.Our dedicated group ABORTION WOMEN’S CLINIC +27730423979 IN women clinic we believe that every woman should be able to make choices in her pregnancy. Our job is to provide compassionate care, safety,affordable and confidential services. That’s why we have won the trust from all generations of women all over the world. we use non surgical method(Abortion pills) to terminate…Dr.LISA +27730423979women Clinic is committed to providing the highest quality of obstetrical and gynecological care to women of all ages. Our dedicated staff aim to treat each patient and her health concerns with compassion and respect.Our dedicated group of receptionists, nurses, and physicians have worked together as a teamof receptionists, nurses, and physicians have worked together as a team wwww.lisywomensclinic.co.za/
The prostate is an exocrine gland of the male mammalian reproductive system
It is a walnut-sized gland that forms part of the male reproductive system and is located in front of the rectum and just below the urinary bladder
Function is to store and secrete a clear, slightly alkaline fluid that constitutes 10-30% of the volume of the seminal fluid that along with the spermatozoa, constitutes semen
A healthy human prostate measures (4cm-vertical, by 3cm-horizontal, 2cm ant-post ).
It surrounds the urethra just below the urinary bladder. It has anterior, median, posterior and two lateral lobes
It’s work is regulated by androgens which are responsible for male sex characteristics
Generalised disease of the prostate due to hormonal derangement which leads to non malignant enlargement of the gland (increase in the number of epithelial cells and stromal tissue)to cause compression of the urethra leading to symptoms (LUTS
Title: Sense of Taste
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the structure and function of taste buds.
Describe the relationship between the taste threshold and taste index of common substances.
Explain the chemical basis and signal transduction of taste perception for each type of primary taste sensation.
Recognize different abnormalities of taste perception and their causes.
Key Topics:
Significance of Taste Sensation:
Differentiation between pleasant and harmful food
Influence on behavior
Selection of food based on metabolic needs
Receptors of Taste:
Taste buds on the tongue
Influence of sense of smell, texture of food, and pain stimulation (e.g., by pepper)
Primary and Secondary Taste Sensations:
Primary taste sensations: Sweet, Sour, Salty, Bitter, Umami
Chemical basis and signal transduction mechanisms for each taste
Taste Threshold and Index:
Taste threshold values for Sweet (sucrose), Salty (NaCl), Sour (HCl), and Bitter (Quinine)
Taste index relationship: Inversely proportional to taste threshold
Taste Blindness:
Inability to taste certain substances, particularly thiourea compounds
Example: Phenylthiocarbamide
Structure and Function of Taste Buds:
Composition: Epithelial cells, Sustentacular/Supporting cells, Taste cells, Basal cells
Features: Taste pores, Taste hairs/microvilli, and Taste nerve fibers
Location of Taste Buds:
Found in papillae of the tongue (Fungiform, Circumvallate, Foliate)
Also present on the palate, tonsillar pillars, epiglottis, and proximal esophagus
Mechanism of Taste Stimulation:
Interaction of taste substances with receptors on microvilli
Signal transduction pathways for Umami, Sweet, Bitter, Sour, and Salty tastes
Taste Sensitivity and Adaptation:
Decrease in sensitivity with age
Rapid adaptation of taste sensation
Role of Saliva in Taste:
Dissolution of tastants to reach receptors
Washing away the stimulus
Taste Preferences and Aversions:
Mechanisms behind taste preference and aversion
Influence of receptors and neural pathways
Impact of Sensory Nerve Damage:
Degeneration of taste buds if the sensory nerve fiber is cut
Abnormalities of Taste Detection:
Conditions: Ageusia, Hypogeusia, Dysgeusia (parageusia)
Causes: Nerve damage, neurological disorders, infections, poor oral hygiene, adverse drug effects, deficiencies, aging, tobacco use, altered neurotransmitter levels
Neurotransmitters and Taste Threshold:
Effects of serotonin (5-HT) and norepinephrine (NE) on taste sensitivity
Supertasters:
25% of the population with heightened sensitivity to taste, especially bitterness
Increased number of fungiform papillae
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Ve...kevinkariuki227
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journeygreendigital
Tom Selleck, an enduring figure in Hollywood. has captivated audiences for decades with his rugged charm, iconic moustache. and memorable roles in television and film. From his breakout role as Thomas Magnum in Magnum P.I. to his current portrayal of Frank Reagan in Blue Bloods. Selleck's career has spanned over 50 years. But beyond his professional achievements. fans have often been curious about Tom Selleck Health. especially as he has aged in the public eye.
Follow us on: Pinterest
Introduction
Many have been interested in Tom Selleck health. not only because of his enduring presence on screen but also because of the challenges. and lifestyle choices he has faced and made over the years. This article delves into the various aspects of Tom Selleck health. exploring his fitness regimen, diet, mental health. and the challenges he has encountered as he ages. We'll look at how he maintains his well-being. the health issues he has faced, and his approach to ageing .
Early Life and Career
Childhood and Athletic Beginnings
Tom Selleck was born on January 29, 1945, in Detroit, Michigan, and grew up in Sherman Oaks, California. From an early age, he was involved in sports, particularly basketball. which played a significant role in his physical development. His athletic pursuits continued into college. where he attended the University of Southern California (USC) on a basketball scholarship. This early involvement in sports laid a strong foundation for his physical health and disciplined lifestyle.
Transition to Acting
Selleck's transition from an athlete to an actor came with its physical demands. His first significant role in "Magnum P.I." required him to perform various stunts and maintain a fit appearance. This role, which he played from 1980 to 1988. necessitated a rigorous fitness routine to meet the show's demands. setting the stage for his long-term commitment to health and wellness.
Fitness Regimen
Workout Routine
Tom Selleck health and fitness regimen has evolved. adapting to his changing roles and age. During his "Magnum, P.I." days. Selleck's workouts were intense and focused on building and maintaining muscle mass. His routine included weightlifting, cardiovascular exercises. and specific training for the stunts he performed on the show.
Selleck adjusted his fitness routine as he aged to suit his body's needs. Today, his workouts focus on maintaining flexibility, strength, and cardiovascular health. He incorporates low-impact exercises such as swimming, walking, and light weightlifting. This balanced approach helps him stay fit without putting undue strain on his joints and muscles.
Importance of Flexibility and Mobility
In recent years, Selleck has emphasized the importance of flexibility and mobility in his fitness regimen. Understanding the natural decline in muscle mass and joint flexibility with age. he includes stretching and yoga in his routine. These practices help prevent injuries, improve posture, and maintain mobilit
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journey
CS 17-18 Management of Upper Respiratory Tract Disorders (1).pptx
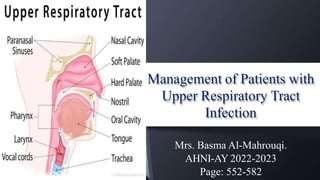
1. Management of Patients with
Upper Respiratory Tract
Infection
Mrs. Basma Al-Mahrouqi.
AHNI-AY 2022-2023
Page: 552-582
2. Objectives
Compare the upper and lower pulmonary infections with
regard to its causes, clinical manifestations, assessment
findings, medical, surgical, nursing management,
complications, and prevention.
Utilize the nursing process as a framework for care of patients
with upper airway infection and patients undergoing
laryngectomy.
3. TOPICS
UpperAirway Infections:
• Viral Rhinitis (Common Cold).
• Acute & Chronic Pharyngitis.
• Acute and Chronic Tonsillitis.
Trauma of the Upper RespiratoryAirway:
• Epistaxis.
• Cancer of the Larynx.
7. Viral Rhinitis
• Most frequent viral infection in the
general population.
• Common cold - URI that is self-limited
& caused by virus.
Causes:
• Influenza (flu), Rhinovirus, Corona,
adenovirus (200 viruses).
• Cold - infectious, acute inflammation of
the mucous membranes of the nasal cavity
8. Viral Rhinitis
• An acute upper respiratory infection (URI).
• Rhinitis, pharyngitis, and laryngitis distinguish the sites of the
symptoms.
• Highly contagious - virus shed for about 2 days before the
symptoms appear & during the first part of the symptomatic phase.
• Rhinoviruses - occur in the early fall and spring.
• Other viruses - cause winter colds.
• Seasonal changes in relative humidity.
• Most common cold: humidity is low, in the colder months of the year.
12. Nursing Management
• Teach how to break the chain of infection:
– Appropriate hand hygiene measures - the most effective
measure to prevent transmission of organisms.
– The use of tissues to avoid the spread of the virus
through coughing and sneezing.
– Cough or sneeze into the upper arm if tissues are not
readily available.
• Instruct about methods to treat symptoms.
12
13. Acute Pharyngitis
• Sudden painful inflammation of the
pharynx, the back portion of the throat
(posterior third of the tongue, soft palate,
and tonsils.
• Commonly referred to as sore throat.
• Due to environmental exposure to viral
agents and poorly ventilated rooms.
• incidence of viral pharyngitis peaks
during winter and early spring in regions
that have warm summers and cold
winters.
13
14. Etiology of Pharyngitis
• Viral - influenza virus, adenovirus, Epstein Barr, Herpes simplex.
– Most common.
– Spreads in droplets of coughs & sneezes.
– Unclean hands due to contaminated fluids.
• Bacterial - groupAbeta-hemolytic Streptococcus (GABHS):
– streptococcus pharyngitis, strep throat.
• Groups B & G streptococcus:
- Mycoplasma pneumoniae, Neisseria gonorrhoeae, and C-
Pneumoniae.
14
15. Clinical Manifestations
• Fiery red pharyngeal membrane & tonsils.
• Lymphoid follicles (swollen and flecked with white-
purple exudates).
• Enlarged & tender cervical lymph nodes.
• Fever & malaise, sore throat.
• Scarlatina forms a rash with urticarial–scarlet fever.
15
A. Redness and vascularity of the pillars and
uvula are mild to moderate
B. Redness is diffuse and intense
17. Medical
Management
• Antimicrobials agents in cases of bacterial infections:
– Penicillin - treatment of choice – 5 days.
– Macrolides –Azithromycin once for 3 days.
– Cephalosporin - Cefuroxime – 5 or 10 days.
– Analgesics – aspirin & acetaminophen.
– Gargles with benzocaine.
• Nutritional management:
– Liquid or soft diet.
– Cool beverages, warm liquids, frozen desserts.
– Encourage to drink 2-3 liter fluids if tolerable.
– I.V. Fluids 17
18. Nursing Management
• Instruct to have plenty of rest.
• Examine the skin once or twice daily for possible rash,
because acute pharyngitis may precede some other
communicable diseases (i.e. rubella).
• Warm saline gargles.
• Drinking warm liquids.
• Encourage oral care and changing toothbrushes.
• Emphasize on full course of antibiotics- to
prevent nephritis & rheumatic fever.
• Ice collar.
• Preventive measures.
18
19. Chronic Pharyngitis
• Persistent inflammation of the
pharynx.
Etiology:
• Adults working in dusty
surroundings.
• Use their voice to excess.
• Suffer from chronic cough.
• Habitually use alcohol and tobacco.
19
20.
21. Clinical Manifestations
• Constant sense of irritation.
• Fullness in the throat.
• Mucus collection &
expelled by coughing.
• Difficulty in swallowing
• Intermittent postnasal drip.
• Avoid exposure to irritants.
Correcting upper respiratory,
cardiac, and pulmonary conditions.
• Nasal sprays: (Phenylephrine) to
relieve nasal congestion.
• Antihistamines decongestant: -
Pseudoephedrine.
• Analgesics: aspirin or
acetaminophen.
• Tonsillectomy. 21
Medical Management
22. Nursing Management
• Teach patient to :
– Avoid smoking & tobacco, and alcohol.
– Minimize exposure to cold or
environmental or occupational pollutants:
• Wear disposable face mask.
– Drink plenty of fluids.
– Have warm saline gargles.
– Take Lozenges - keep the throat moist.
22
23. Tonsillitis
• Tonsils - composed of lymphatic tissue which
frequently serve as the site of acute infection.
• Chronic - less common and may be mistaken for
allergy, asthma, and rhinosinusitis.
• Infection of the adenoids frequently accompanies
acute tonsillitis.
Etiology:
• Bacteria - GABHS, the most common.
• Viral - Epstein-Barr - most common.
• Can occur in adults.
23
25. Assessment/
Diagnostic Findings
– Physical assessment and history
Rapid Antigen Detection Testing
(RADT)
– Throat Swab Culture
– Comprehensive audiometric exam
Cytomegalovirus infection
- differential diagnosis for
HIV, hepatitisA, and rubella
Adenoiditis- recurrent
of suppurative otitis media
result in hearing loss.
25
26. Tonsillitis:
Medical Management
• Antibiotics ( Penicillin, Cephalosporin).
• Teach patients to complete medication courses.
Bacterial
Infections
• Increased fluid intake, Analgesics.
• Salt water gargles & rest.
Supportive
measures
• Repeated episodes of tonsillitis despite antibiotic therapy.
• Hypertrophy of the tonsils could cause obstruction and
obstructive sleep apnea.
• Chronic nasal airway obstruction, chronic rhinorrhea.
Tonsillectomy
&
Adenoidectomy
27. Providing Postoperative
Care
Educating Patients about
Self care
• Alkaline mouthwashes and warm saline
solution - removal of thick mucus and
halitosis.
• Sore throat, stiff neck, minor ear pain
vomiting – 1st 24 hours.
• Adequate diet with soft foods &Avoid
spicy, hot, acidic, or rough foods.
• Restrict milk and milk products &
maintain good hydration.
• Use ofa cool mist vaporizer or humidifier
• Avoid vigorous tooth brushing or
Gargling.
• Avoid smoking and heavy lifting or
exertion for 10 days.
• Continuous nursing observation (risk of
hemorrhage).
• Observe for frequent swallowing
(indicates hemorrhage).
• Position patient in a prone, with the
patient’s head, turned to the side (allows
drainage from the mouth and pharynx).
• Do not remove the oral airway until
the patient’s gag and swallowing reflexes
have returned.
• Apply an ice collar to the neck & Provide
• A basin and tissues & Give water and ice chips.
• Instructed to refrain from too much talking and
coughing.
29. Epistaxis
(Nose Bleed)
• A hemorrhage from the
nose, caused by the
rupture of tiny, distended
vessels in the mucous
membrane of any area of
the nose.
30. Epistaxis (Nosebleed)
• Most common site is - Anterior
septum, where three major blood
vessels enter the nasal cavity.
• (1) Anterior ethmoidal artery on the
forward part of the roof (Kiesselbach’s
plexus).
• (2) Sphenopalatine artery in the
posterosuperior region.
• (3) Internal maxillary branches (the
plexus of veins located at the back of
the lateral wall under the inferior
turbinate).
32. Medical Management
Initial Treatment:
Apply direct pressure.
Uncontrolled bleeding:
Visible bleeding sites may be cauterized with silver nitrate or
electrocautery (high-frequency electrical current).
A cotton tampon may be used to try to stop the bleeding.
Educating about self-care
Avoid vigorous exercise for several days,Avoid hot or spicy foods and tobacco Avoid straining,
high altitudes, and nasal trauma, prevent drying of the nasal passages.
• Sits upright with the head tilted forward
(prevents swallowing & aspiration of blood )
• Pinch the soft outer portion of the nose
against the midline septum for 5 or 10
minutes continuously
• Apply nasal decongestants
Vasodilation
33. Medical Management
Packing to control bleeding from the
posterior nose (Balloon- inflated
catheter).
• A. Catheter is inserted and packing is
attached.
• B. Packing is drawn into position as the
catheter is removed.
• C. Strip is tied over a bolster to hold the
packing in place with an anterior pack
installed “accordion pleat” style.
• D. Alternative method, using a balloon
catheter instead of gauze packing.
Antibiotics – to prevent iatrogenic sinusitis and sepsis
34. Nursing Management
• Assess vital signs.
• Assess amount of bleeding.
• Give assurance in a calm and efficient manner.
• Teach to avoid vigorous exercise, avoid hot and spicy
foods, avoid nasal blowing, straining, high altitude and
nasal trauma.
• Administer IV crystalloid solution as prescribed.
35
35. Cancer of the Larynx
• Half of the neck and head cancer.
• Most common in people Older than 65.
• 4x more common in men.
• 5-year survival rate – 32% - 90%.
• Classified as Squamous cell carcinoma.
• 55% with lymph node involvement.
• Carcinogens: Tobacco (smoke,
smokeless) and asbestos, paint fumes,
wood dust, chemicals, tar products,
leather, and metals.
37. Clinical Manifestations
Initial symptoms
• Hoarseness - tumor
impedes the action of
the vocal cords
during speech
• Persistent cough
• Sore throat or pain,
burning in throat
• Lump in neck
Later symptoms
• Dysphagia
• Dyspnea
• Unilateral nasal
obstruction or
discharge
• Persistent hoarseness
• Persistent ulceration
• Foul breath
Metastasis
• Unintentional weight
loss
• General debilitated
state
• Cervical
Lymphadenopathy
• Pain radiating to ear
38. Cancer of the Larynx
Assessment and Diagnostic Findings
• History & Physical Examination.
• Indirect / direct laryngoscopy.
• Mobility of the vocal cords.
• Fine NeedleAspiration Biopsy
(FNAB).
• Barium swallow.
• Endoscopy, Laryngoscopy.
• CT or MRI Scan – regional adenopathy.
• PET Scan.
39
39. Cancer of Larynx Assessment
Direct laryngoscopy
(under LA/ GA)
To evaluate all
areas of the
larynx
CT and MRI
To stage and
determine the
extent of a tumor
Post Tx….to
detect a
recurrence
40. Medical Management
Goals:
• Cure; preservation of safe, effective swallowing; preservation of useful voice; and
avoidance of permanent tracheostomy.
Treatment Options:
• Surgery - Partial vs. total laryngectomy – Stage 3 & 4.
• External Beam Radiation therapy & conservation surgery – Stage 1 & 2.
• Adjuvant chemo-radiation therapy.
• Speech therapy.
• Artificial larynx.
41
41. • Vocal Cord Stripping - used to treat
dysplasia, hyperkeratosis, and
leukoplakia and is often curative for
these lesions; involves removal of the
mucosa of the edge of the vocal cord,
using an operating microscope.
• Cordectomy - excision of the vocal cord,
is usually performed via transoral laser;
used for lesions limited to the middle
third of the vocal cord.
Surgical Management
42. • Laser microsurgery - well known to have
several advantages for the treatment of early
glottic cancers; shorter Treatment and
recovery with fewer side effects, and
treatment may be less costly.
• Partial laryngectomy (laryngofissure–
thyrotomy) - used in the early stages of
cancer in the glottic area when only one vocal
cord is involved; associated with a very high
cure rate; A portion of the larynx is removed,
along with one vocal cord and the tumor; all
other structures remain.
Surgical Management
43. •
•
A. Normal airflow
B. Airflow after total laryngectomy
Changes in Airflow with
Total Laryngectomy
Total laryngectomy
• Complete removal of the larynx
(total laryngectomy) can provide a
cure for most advanced laryngeal
cancers.
• the laryngeal structures are
removed, including the hyoid
bone, epiglottis, cricoid cartilage,
and two or three rings of the
trachea.
• The tongue, pharyngeal walls,
and most of the trachea are
preserved.
• results in permanent loss of the
voice and a change in the airway,
requiring a permanent
tracheostomy.
44. Speech Therapy
Esophageal Speech
The patient needs the ability to compress
air into the esophagus and expel
it, setting off a vibration of the pharyngeal
esophageal segment for
esophageal speech.
Artificial Larynx
If esophageal speech is not successful, or until
the patient masters the
technique, an electric larynx may be used for
communication. This batterypowered
apparatus projects sound into the oral cavity.
When the mouth
forms words (articulation), the sounds from
45. Speech Therapy
Esophageal Speech -The patient needs the ability to
compress air into the esophagus and expel it, setting off a
vibration of the pharyngeal esophageal segment for
esophageal speech.
Artificial Larynx - an electric larynx that is battery powered
apparatus that projects sound into the oral cavity. When the
mouth forms words (articulation), the sounds from the electric
larynx become audible words.
Tracheoesophageal puncture - A valve is placed in the tracheal
stoma to divert air into the esophagus and out the mouth,
once the puncture is surgically created and has healed, a voice
prosthesis (Blom- Singer) is fitted over the puncture site.
46. Nursing Interventions
Provide Preoperative Patient education
• If a complete laryngectomy is planned, the patient must understand that the NATURALVOICE
WILLBE LOST.
– Special training can provide a means for communicating.
– Until training is started, communication will be possible by using the:
• Call light.
• Writing.
• Using a special communication board.
– Give adequate time to communicate his or her needs.
– Be aware that the patient may become impatient and angry when not understood.
47. Nursing Interventions
Teaching Patient Preoperatively
• Review equipment and treatments for postoperative care (tracheostomy care,
etc) with the patient and family.
• Teach about coughing and deep breathing exercise.
• Provide the patient and family with opportunities to ask questions, verbalize
feelings, and discuss perceptions.
• Promote feeling of comfort - listening to music, reading, guided imagery,
meditation – to reduce anxiety.
48. Maintaining a Patent Airway
To decrease surgical edema and
promotes lung expansion
• Position the patient in the semi-Fowler’s or Fowler’s
position after recovery from anesthesia.
• Observe the patient for restlessness, labored
breathing, apprehension, increased pulse rate &
decreasing saturation.
To identify possible respiratory or
circulatory problems
To detect impending complications
• Assess the patient’s lung sounds and reports changes
• Encourage the patient to turn, cough, and take deep
breaths.
• Careful suctioning without disruption of sutures.
To remove secretions
• Encourage and assist the patient with early
Ambulation.
To prevent atelectasis, pneumonia,
and deep vein thrombosis
49. • Advice:
– Avoid sweet foods as they increase salivation.
– Rinse mouth with warm water/mouthwash after oral feeding.
Promoting Adequate
Nutrition & Hydration
• Postoperatively, the patient may not be permitted to eat or drink for several days (7 days):
– IV fluids.
– Enteral feedings through a nasogastric or gastrostomy tube.
– Parenteral nutrition.
To avoid irritation to the sutures.
To reduce the risk of aspiration.
• Oral feeding is initiated only after a swallow study (radiology procedure).
• Provide thick liquids.
Stay with patient during initial oral feedings
Keep a suction set-up at the bedside
50. Instruct the patient and caregiver:
– Perform suctioning
– Gently cover the stoma with a loose plastic bib, or even a hand, when
showering or bathing to prevent water from entering the stoma.
– Cover the stoma with a loose-fitting, not tight, cloth to protect it.
– Keep his/her house humidified to prevent irritation of
the stoma that can occur in low humidity.
– Avoid swimming, because it's possible for water to enter the stoma and then
enter the patient's lung, causing him/her to drown without submerging
his/her face.
Teaching Home &
Community Based Care