Downloaded 125 times


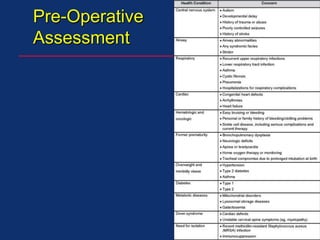
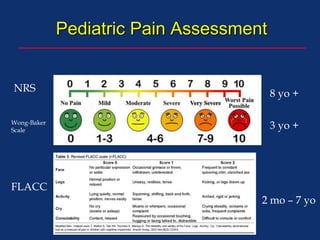
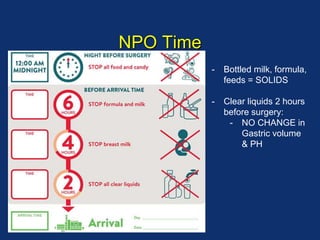
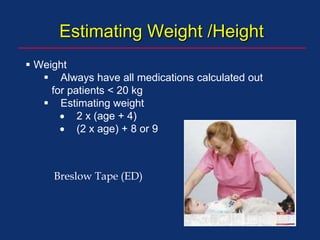
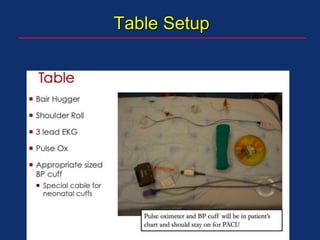
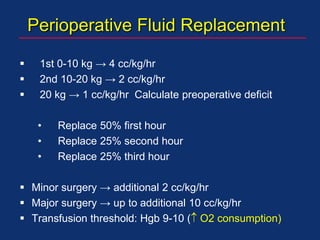
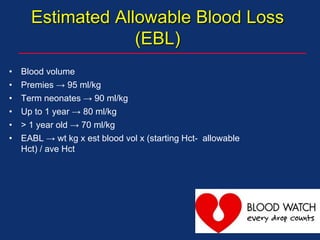
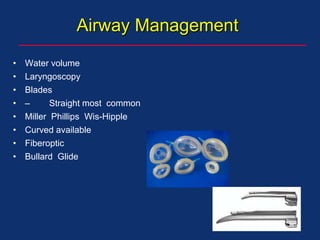
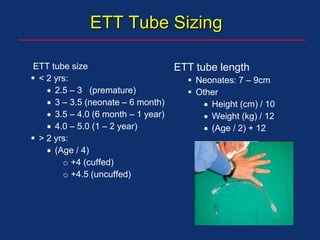
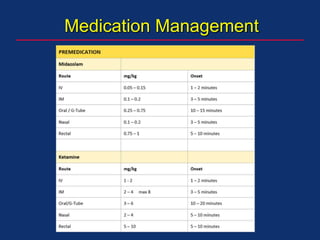
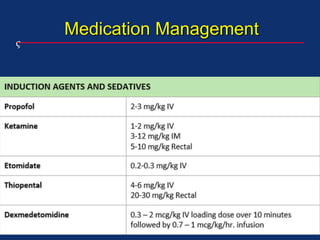
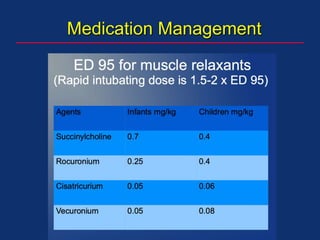
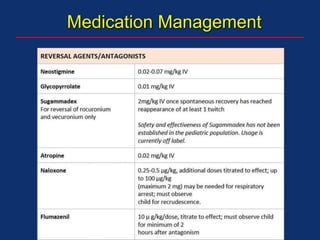



The document discusses pediatric anesthesia, covering essential topics such as anesthetic management for infants and children, pre-operative assessment, and physiological differences between neonates and adults. It includes specific guidelines related to airway management, drug dosing, fluid replacement, and post-operative care in children. Additionally, the document references various neonatal emergencies and conditions that require specialized care.





![The basics of peds anesthesia [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/thebasicsofpedsanesthesiaautosaved-111017032903-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

