Download to read offline
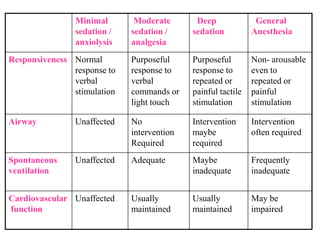





The document outlines methods for managing behavior in pediatric dentistry, emphasizing the importance of addressing fear and anxiety in young patients. It discusses non-pharmacological and pharmacological behavior management techniques, detailing specific sedation levels and administration routes, including oral, intramuscular, intravenous, and nitrous oxide inhalation. Additionally, it highlights the indications, contraindications, and safety recommendations for sedation, as well as the effects of sedative agents on children.























































































