Downloaded 2,815 times
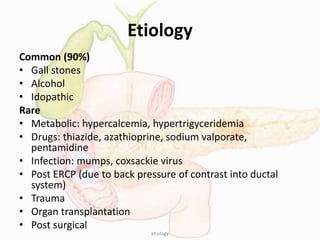
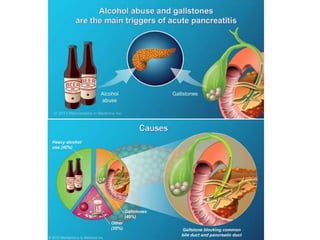
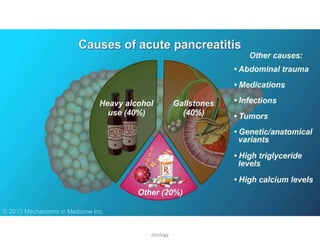
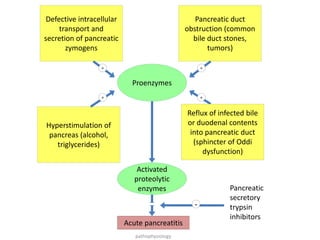
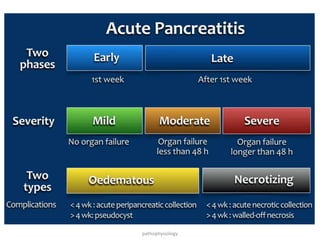
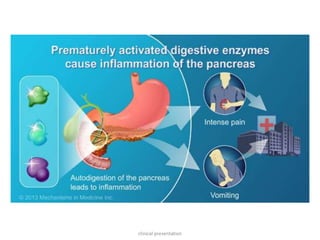

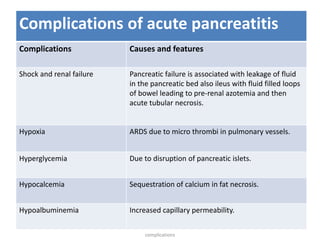
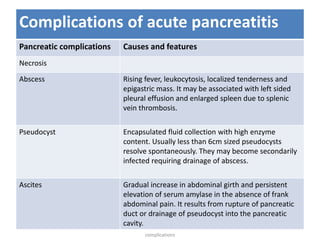
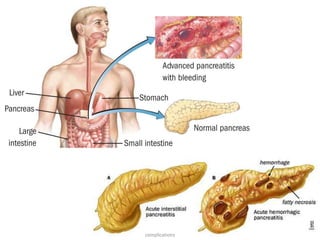
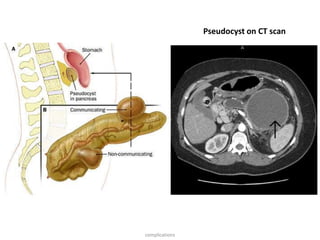
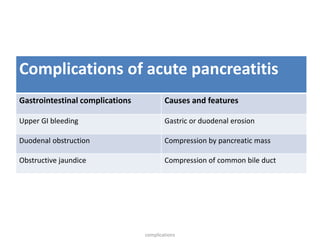
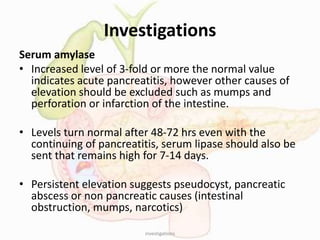

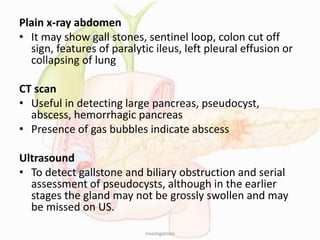
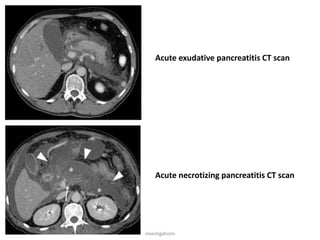
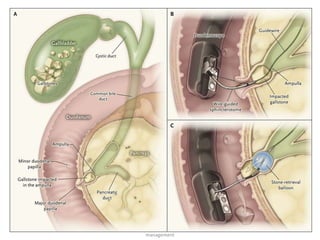


Acute pancreatitis is a condition where pancreatic enzymes leak into the pancreas and cause its auto-digestion. Common causes include gallstones, alcohol use, and idiopathic factors. Patients present with epigastric pain radiating to the back that is exacerbated by eating or lying down. Lab tests show elevated pancreatic enzymes and imaging shows changes to the pancreas. Treatment is supportive with NPO, IV fluids, pain control and monitoring for complications like necrosis, pseudocysts, shock and respiratory failure. Severe cases may require ERCP, surgery or drainage procedures.






















































































