Downloaded 1,449 times
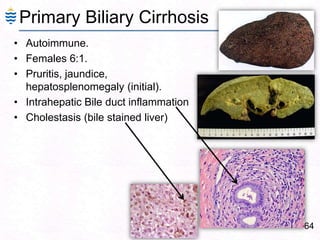
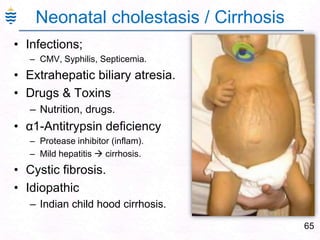



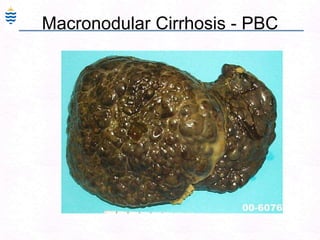
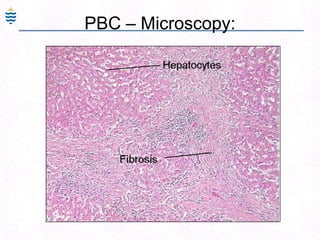

Here are brief summaries of the requested liver conditions: - Primary Biliary Cirrhosis (PBC) and Primary Sclerosing Cholangitis (PSC): - PBC affects small bile ducts, PSC affects large bile ducts - PBC more common in females, PSC more common in males - PBC associated with autoimmune diseases, PSC associated with IBD - Wilson's disease involves copper accumulation in liver due to ceruloplasmin defect - Alpha-1 antitrypsin deficiency results in decreased protease inhibition and liver damage - Hemochromatosis involves iron overload due to HFE gene mutation - Hemosiderosis is iron overload from other causes like























































































