Downloaded 273 times







































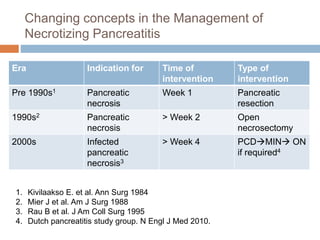



































































This document provides an overview of pancreatic surgery and management of pancreatic conditions. It discusses the anatomy of the pancreas, classification and management of acute pancreatitis including necrotizing pancreatitis. It covers the indications, timing and approaches for intervention in infected pancreatic necrosis, including radiologic drainage, minimally invasive techniques like VARD and nephroscopic debridement, and open necrosectomy. It also summarizes the principles and techniques of surgical management of pancreatic cancer.























































































