Downloaded 166 times
![Introduction
Usually secondary to widespread nodal disease
Gastrointestinal tract – most common extra-nodal site
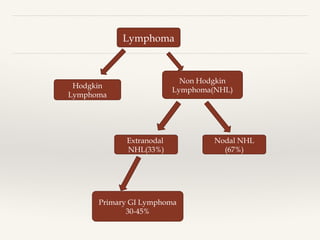
Primary gastrointestinal lymphoma
- 1-4% of all GI malignancies
- 10-15% of all lymphomas
- 30-40% of all extra nodal lymphomas
Majority – Non Hodgkins Lymphoma [B cell- 90%]
Most common site – stomach (60-65%)
Rare sites – esophagus, pancreas, liver](https://image.slidesharecdn.com/crfvptebssg1xasscxow-signature-5ad637fb3c053e41151106d5fd77df1246c520c5662955ecc0b8e683c83dd6d2-poli-181120065426/85/GI-Lymphoma-4-320.jpg)


This document discusses primary lymphomas of the gastrointestinal tract. It begins by providing background on lymphomas and noting that the gastrointestinal tract is a common extra-nodal site. The most common subtypes of primary GI lymphomas are then described, including their typical locations and risk factors. Diagnostic workup, staging systems, treatments, and outcomes are outlined for several subtypes affecting different areas of the GI tract, such as diffuse large B-cell lymphoma and MALT lymphoma in the stomach, and immunoproliferative small intestinal disease. Throughout, key points are illustrated with images and tables.























































































