Downloaded 17 times

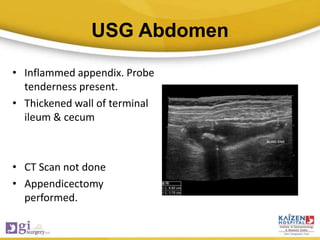

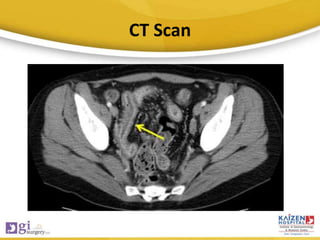
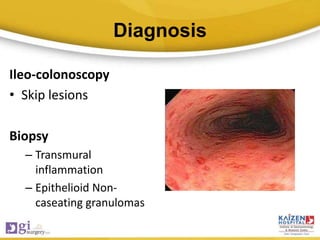
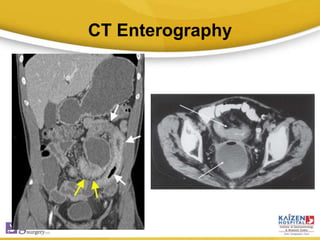

Crohn's disease is a chronic inflammatory bowel disease that can involve any part of the gastrointestinal tract from mouth to anus. It is characterized by periods of remission and relapse. Three case studies are presented where the initial diagnoses were missed, but were later found to be Crohn's disease based on histopathological findings. Key learning points are the importance of thorough history taking, use of appropriate investigations like CT scans and colonoscopy with biopsies to confirm diagnoses, and considering Crohn's disease in cases of recurrent or unusual presentations of conditions like appendicitis and fistula-in-ano. Early diagnosis and treatment with immunomodulators can help manage the disease effectively and preserve bowel function.



















































































