Downloaded 35 times

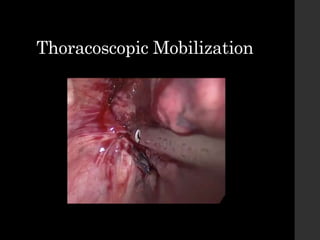


Minimally invasive esophagectomy (MIE) is an evolving technique for treating esophageal cancer that offers advantages over traditional open esophagectomy. MIE uses small incisions and video-assisted thoracic surgery to mobilize the esophagus, allowing for less post-operative pain, quicker recovery times, and reduced pulmonary complications compared to open techniques. While short-term outcomes are improved with MIE, long-term oncological outcomes still need to be defined as surgery aims to completely remove the cancer while preserving quality of life. MIE represents a shift toward less invasive options for esophageal cancer treatment when surgery is required.








































![Esophagus ppt [Autosaved] [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/esophaguspptautosavedautosaved-230203010548-a58d6d4b-thumbnail.jpg?width=640&height=640&fit=bounds)









































