Downloaded 143 times

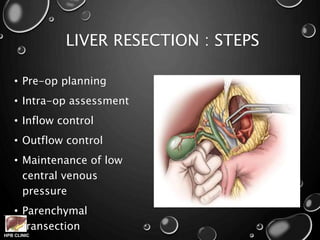
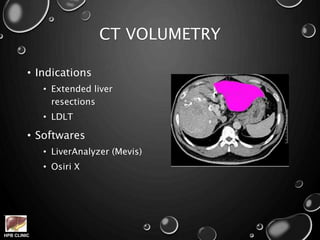
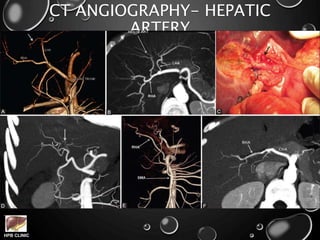
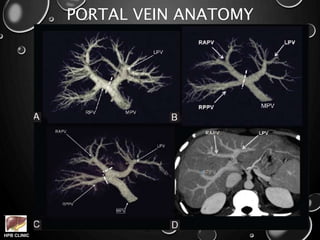
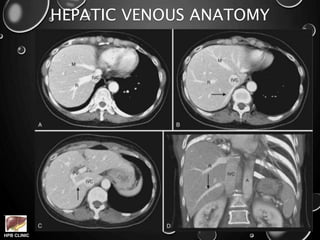
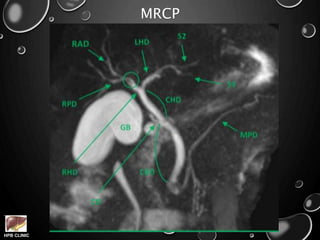
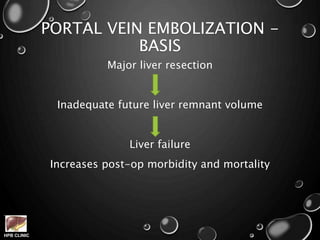
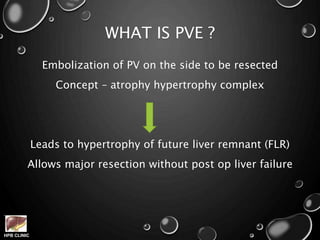


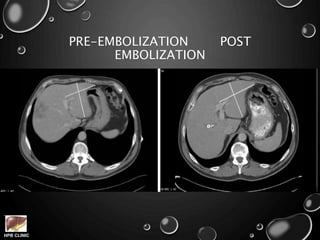
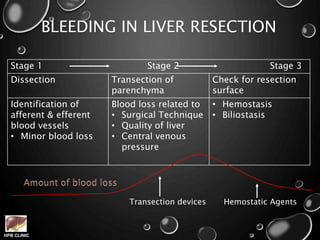
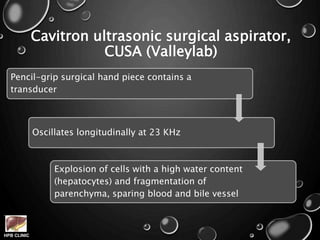

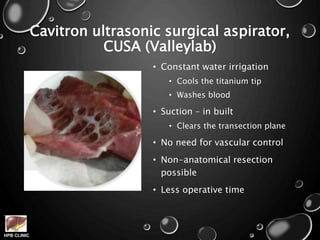



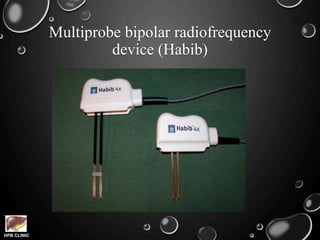
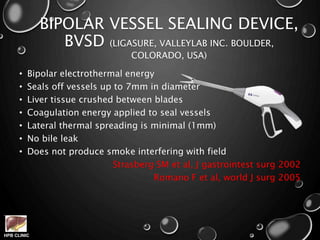
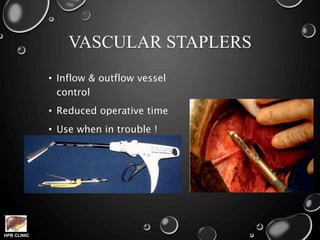



This document summarizes recent advances in liver resection techniques. It discusses improvements in pre-operative planning using CT volumetry and angiography. It also describes intra-operative techniques like portal vein embolization to increase the future liver remnant. New devices for safer liver transection are presented, including waterjet dissection, radiofrequency probes, harmonic devices, and laparoscopic approaches. Overall, recent advances have made liver surgery less morbid with lower blood loss through improved planning and new instrumentation.






























![Hepatic Resection techniques[Autosaved]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hepaticresectionautosaved-1-240310100405-b4ce2794-thumbnail.jpg?width=640&height=640&fit=bounds)










































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)











