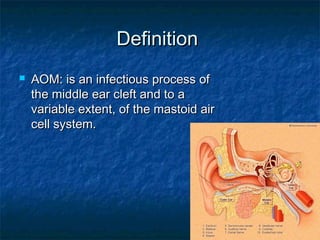
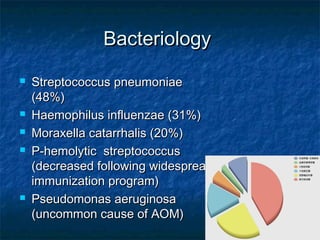
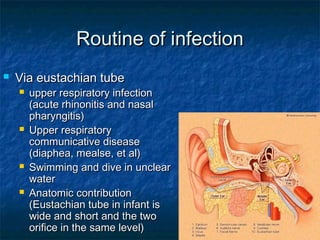
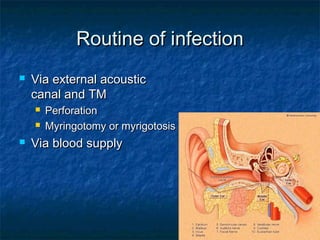
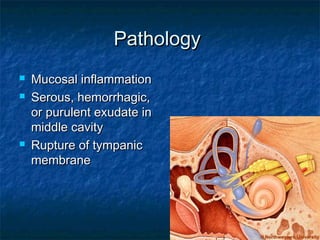
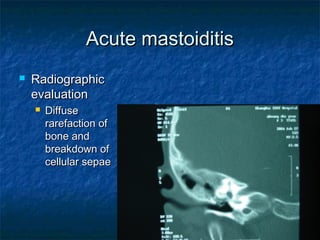
Acute otitis media and mastoiditis are infectious processes of the middle ear and mastoid air cells. Common bacteria include Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis. Acute otitis media symptoms include fever, otalgia, and hearing loss. Physical exam may show bulging of the tympanic membrane. Treatment involves antibiotics for 5-10 days. Acute mastoiditis causes otalgia, fever, and postauricular swelling. Imaging shows bone rarefaction. Treatment requires intravenous antibiotics and may require mastoidectomy.








































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




