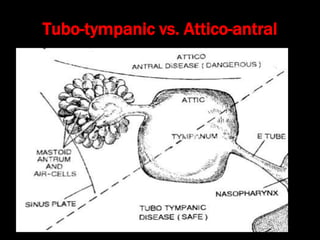
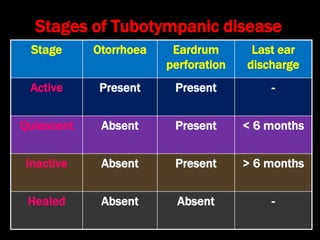
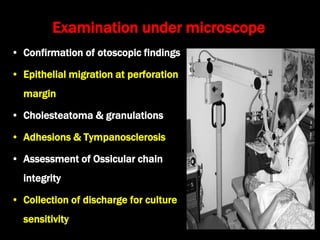
Chronic suppurative otitis media (CSOM) is a pyogenic infection of the middle ear characterized by prolonged ear discharge and hearing loss, primarily involving the tubo-tympanic type. The document discusses the predisposing factors, common bacteria, clinical features, and various treatment methods, including both non-surgical and surgical options to address eardrum perforations and restore hearing. Additionally, detailed examination and investigation procedures are outlined to confirm the diagnosis and monitor treatment effectiveness.

























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


