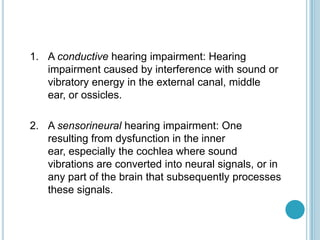
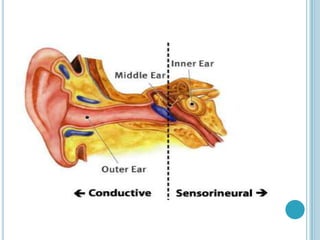
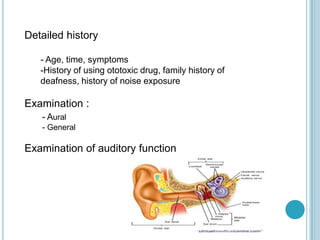
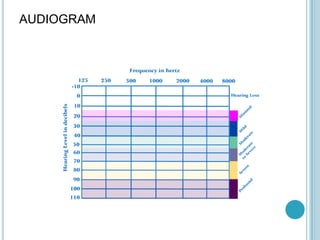
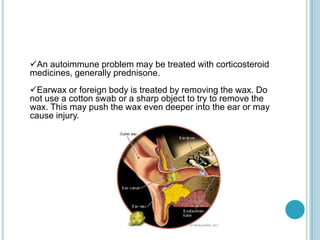
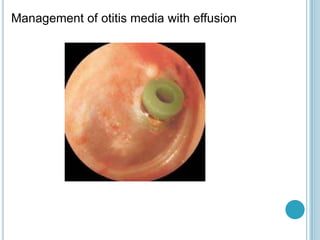
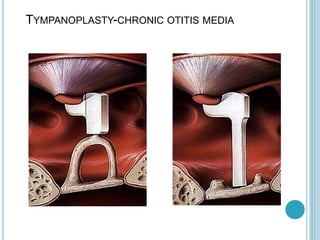
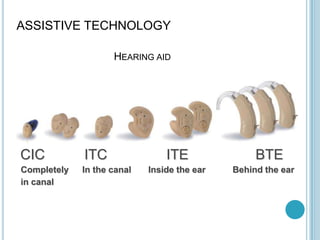
This document provides an overview of assessment and management of deafness in children and adults. It discusses types of hearing impairment, common causes including genetic factors and infections, methods of evaluation such as audiometry, and interventions like hearing aids, cochlear implants, education supports, and protective measures to prevent deafness.