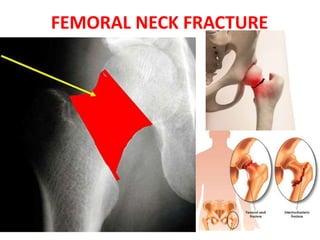
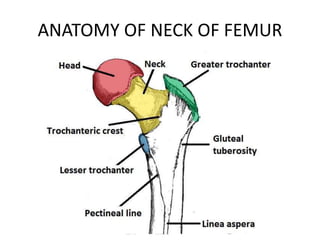
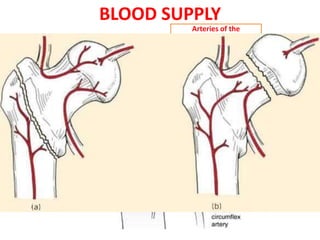
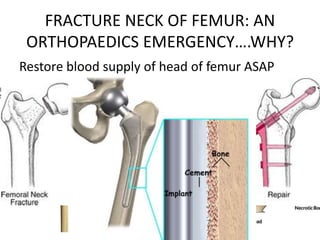
The document discusses a case of a 55-year-old male who suffered a neck of femur fracture following a fall, detailing his symptoms, examination findings, treatment via surgery, and postoperative recovery. It highlights the importance of timely intervention to restore blood supply and outlines the epidemiology, classification, diagnosis, complications such as avascular necrosis, and treatment options for neck of femur fractures. The conclusion emphasizes that these fractures are common and require surgical intervention, while also noting the risks of osteonecrosis.




































![INJURIES AROUND HIP [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/injuriesaroundhipautosaved-240206110505-4ae81da1-thumbnail.jpg?width=640&height=640&fit=bounds)



























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




