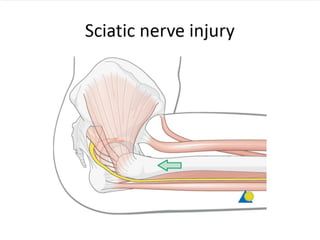
This document summarizes the case of a 41-year-old man who was in a car accident where he hit a tree with his console but did not hit his head. He reported right hip pain after the accident and could not walk or move his right leg. On examination, he had marked tenderness over his right hip with limited and painful range of motion. He was taken to the OR for closed reduction of a posterior hip dislocation under general anesthesia. Potential complications of posterior hip dislocations include osteonecrosis, osteoarthritis, and sciatic nerve injury.







































![Noon conf. [Ext.Worawan]](https://cdn.slidesharecdn.com/ss_thumbnails/ext-161212044740-thumbnail.jpg?width=640&height=640&fit=bounds)













































