Download to read offline

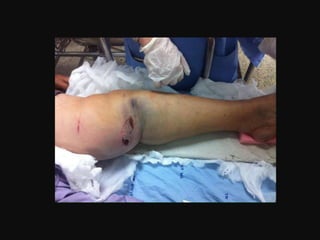
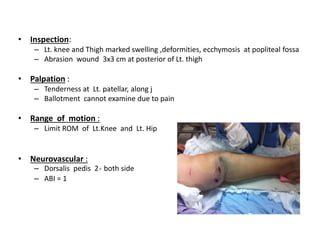




- The patient is a 54-year-old female who was in a motorcycle accident 4 hours prior where her motorcycle was hit on the side causing her to fall and injure her left leg. - On examination, she had swelling and deformity of her left knee and thigh with tenderness and limited range of motion. X-rays showed a posterolateral dislocation of the left knee. - She underwent closed reduction of the knee dislocation. A CTA showed no evidence of vascular injury. She was diagnosed with a posterolateral left knee dislocation and given splinting and pain management.



































![Noon conf. [Ext.Worawan]](https://cdn.slidesharecdn.com/ss_thumbnails/ext-161212044740-thumbnail.jpg?width=640&height=640&fit=bounds)































