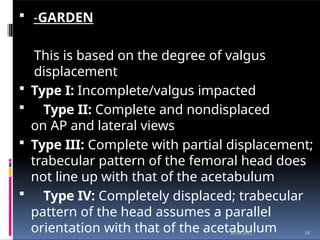
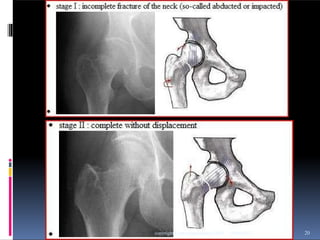
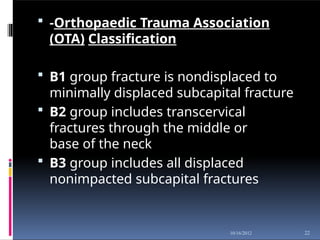
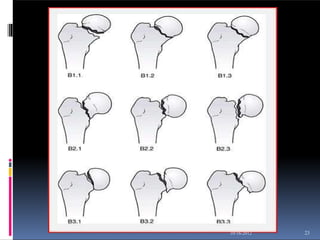
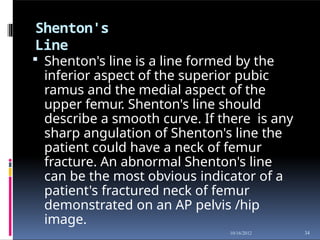
The document outlines femoral neck fractures, covering aspects such as anatomy, mechanisms of injury, classification, clinical presentation, diagnosis, treatment options, and rehabilitation strategies. It emphasizes the importance of understanding the anatomical and pathological characteristics of femoral neck fractures, particularly in elderly patients, and details both surgical and non-surgical treatment approaches. Additionally, it discusses complications and physiotherapy management for post-operative recovery.









![Three to five days postoperative
• Gait train patient, observing weight-bearing precautions. Progress to walker
or crutches. Goal: Establish independent gait with assistive device, using
proper gait pattern on all surfaces and stairs.
• Initiate training in activities of daily living, including bed mobility and
transfers to and from bed and toilet. Goal: Achieve independence with all
transfers.
• Initiate active range of motion/strengthening program. Individualize exercise
programs according to each patient's needs, but generally include the
following.
• Goals: Increase strength of involved extremity; increase independence with
exercise program.
• Supine: hip abduction and adduction, gluteal sets, quadriceps sets,
straight leg raise, hip and knee flexion, short arc quadriceps, internal and
external rotation.
• Sitting: Long arc quadriceps, hip flexion, ankle pumps[16]
.
• When internal fixation is performed, partial weight-bearing is recommended
for a period of 8–10 weeks (according to the radiological evaluation of](https://image.slidesharecdn.com/fractureofneckofthefemur-121016113941-phpapp02-250122222556-b84ce45c/85/fractureofneckofthefemur-121016113941-phpapp02-pptx-47-320.jpg)















![INJURIES AROUND HIP [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/injuriesaroundhipautosaved-240206110505-4ae81da1-thumbnail.jpg?width=640&height=640&fit=bounds)










































