- A 66-year-old Thai Buddhist woman presented to the hospital after falling and injuring her left wrist 2 hours prior.
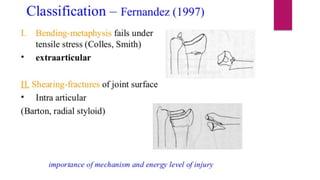
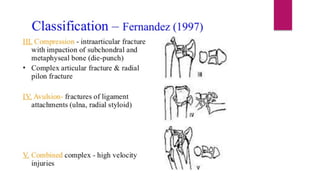
- On examination, her left wrist was tender and swollen with limited range of motion due to pain. X-rays revealed a Fernandez type I fracture of the distal left radius.
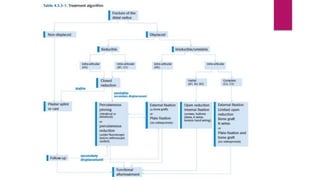
- The diagnosis was a left distal radius fracture, which was managed with sedation, closed reduction, and application of a short arm cast.