Downloaded 50 times

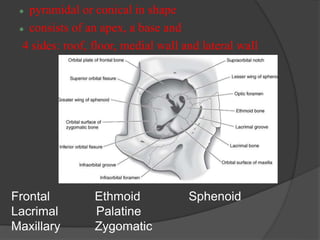
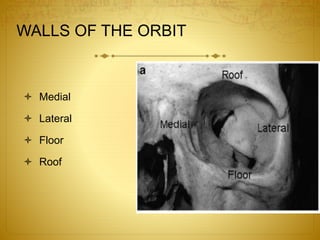
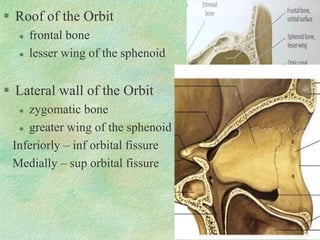
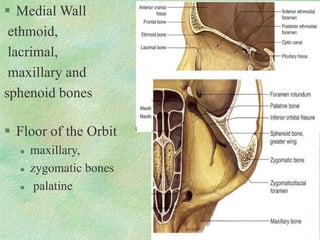
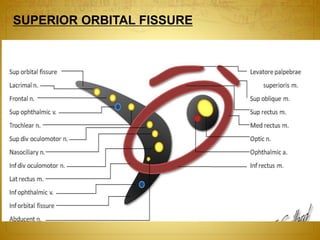
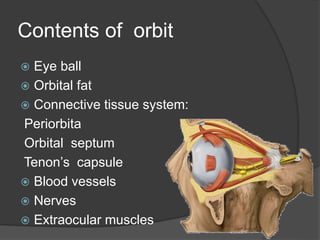
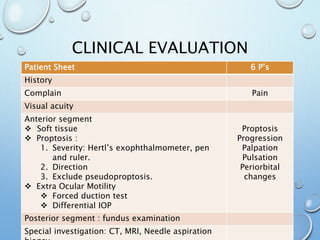


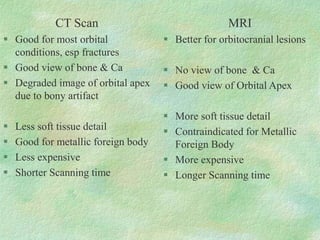
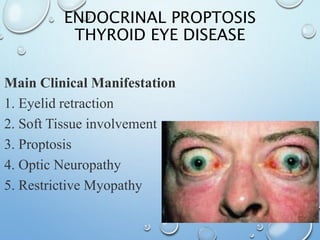


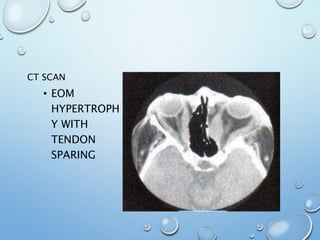
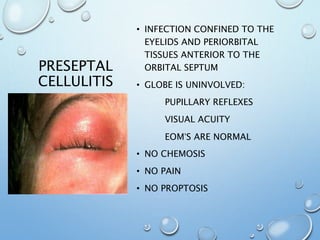
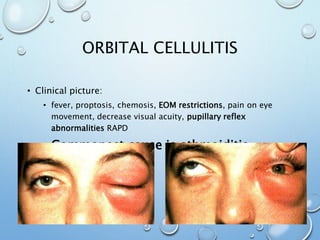
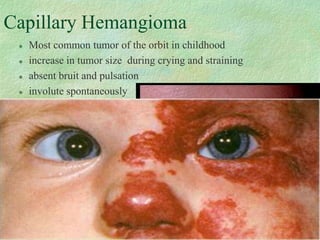
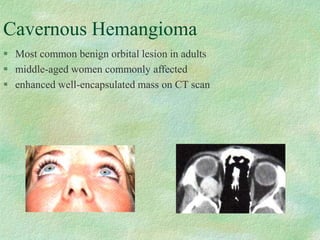
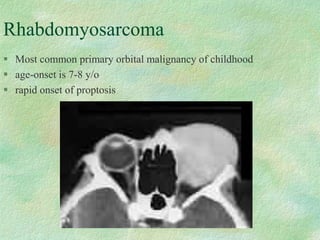
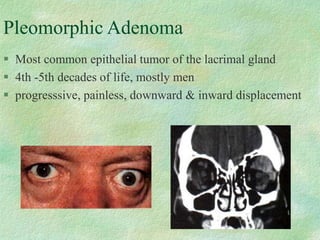
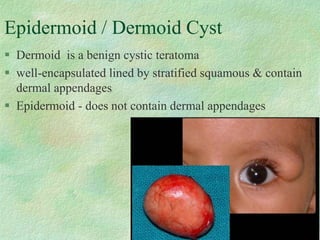
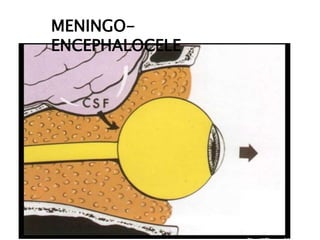
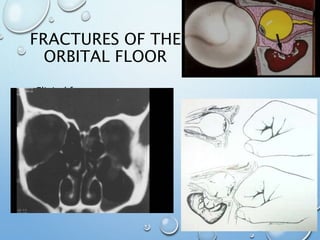
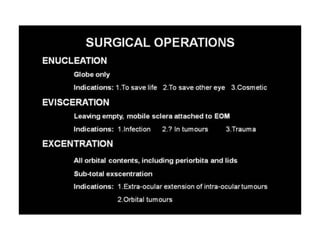


The document provides an overview of orbital anatomy and diseases. It describes the bones that make up the walls of the orbit, as well as the contents of the orbit such as the eyeball, muscles, nerves and blood vessels. Common orbital diseases are discussed including thyroid eye disease, infections, tumors and cysts, and trauma. Clinical evaluation involves assessing features like proptosis, extraocular motility, and imaging studies. Specific conditions like dermoid cysts, hemangiomas and fractures are also outlined.











































































































