Downloaded 1,079 times


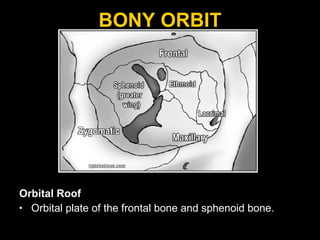
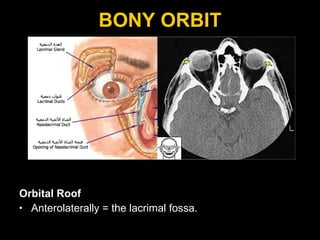
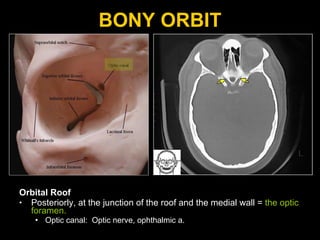
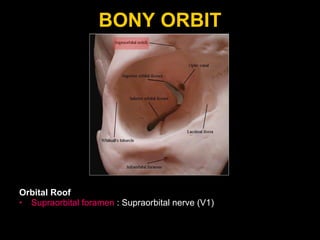
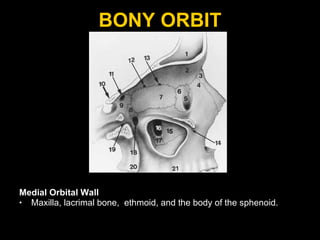
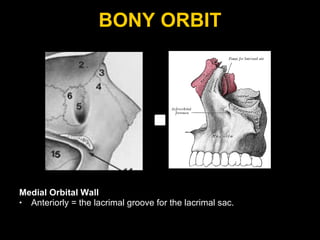
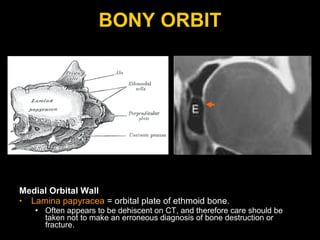
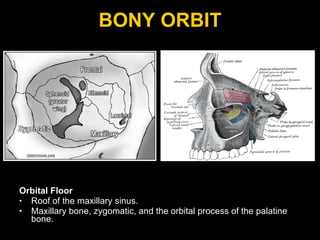
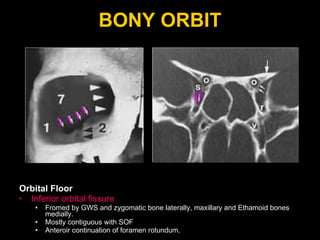
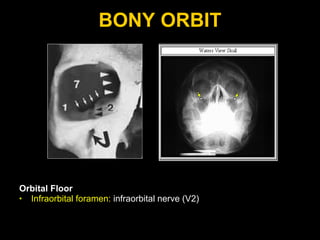
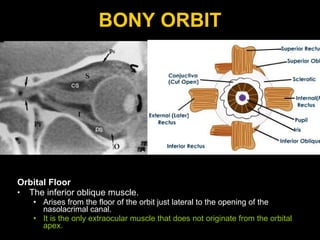
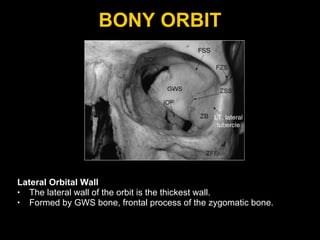
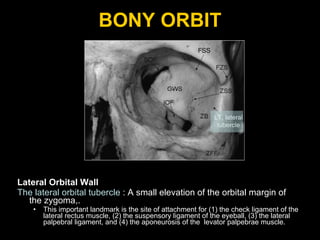
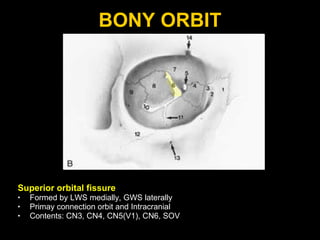
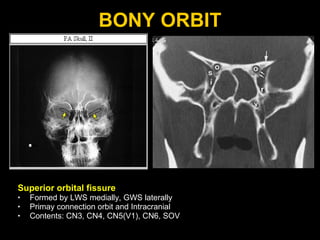
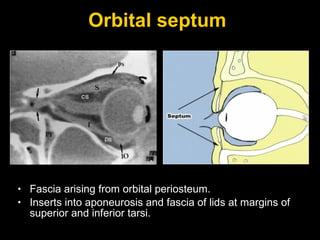
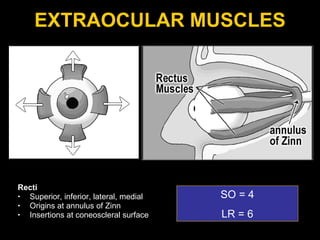
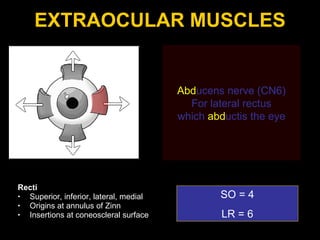
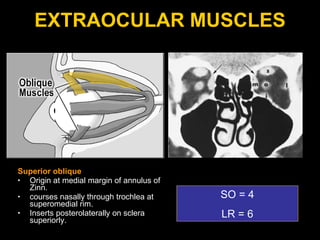
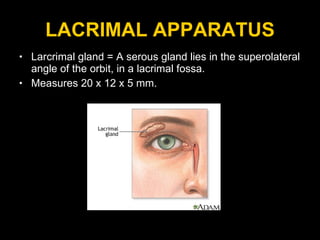
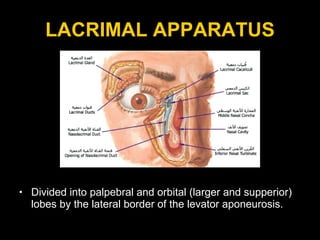
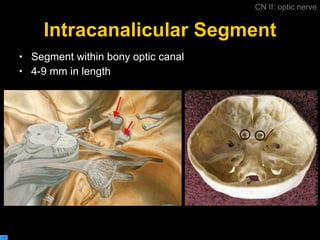
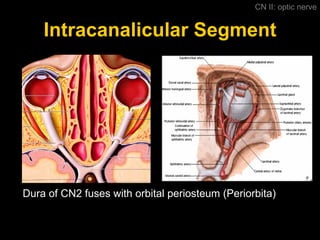
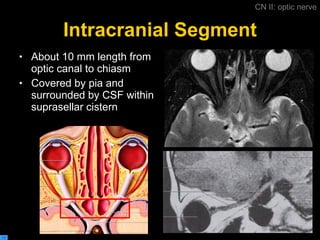
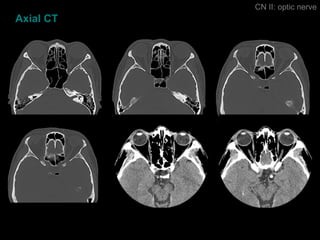
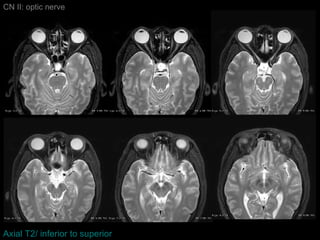


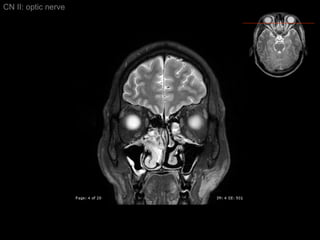
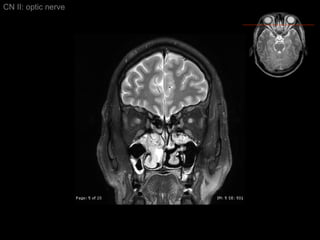

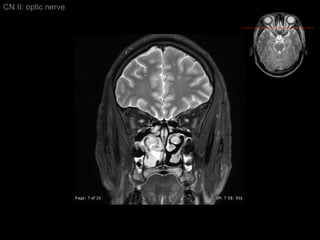


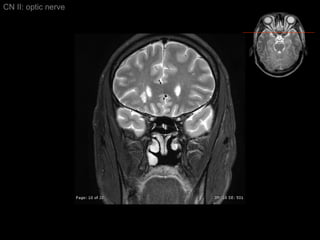






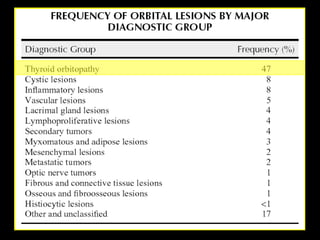


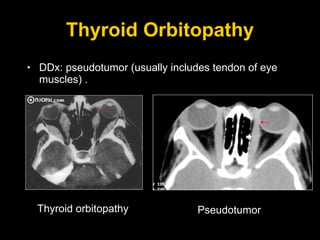
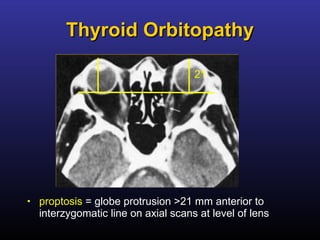
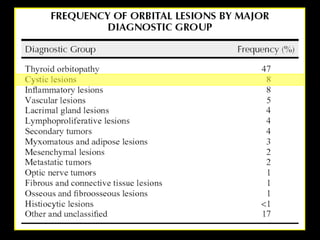



























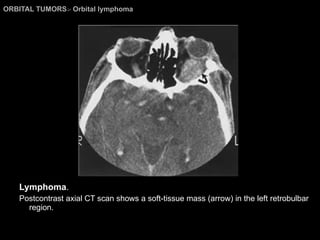
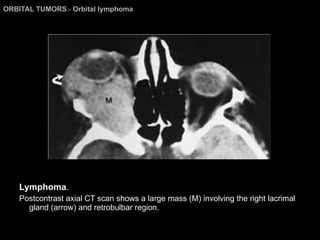







The document describes various anatomical structures of the orbit and eye, including: 1) The bony orbit is formed by the frontal, sphenoid, maxillary, zygomatic, ethmoid, and palatine bones. It contains openings like the optic canal and infraorbital foramen. 2) The extraocular muscles include the four recti and two oblique muscles originating at the orbital apex. 3) The orbit contains the lacrimal gland, eyelids, optic nerve, ophthalmic artery, and ophthalmic veins. 4) Common orbital pathologies discussed include thyroid orbitopathy, dermoid cysts, hematologic cysts, and cholesterol granulomas.



































































































