Download to read offline

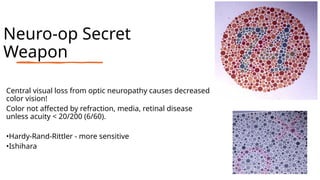
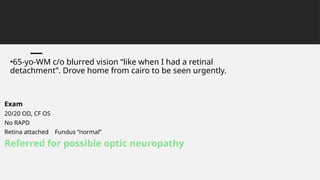
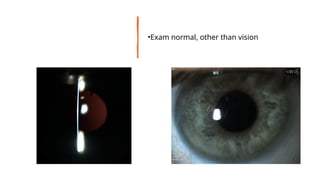
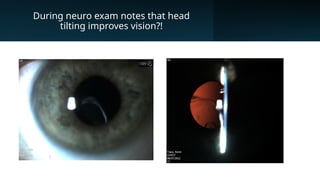
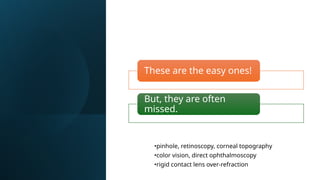

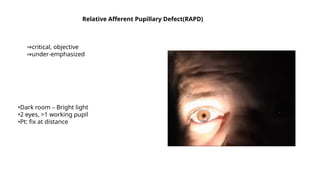


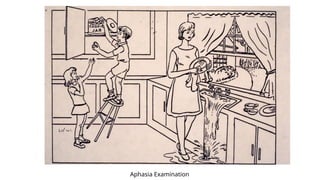
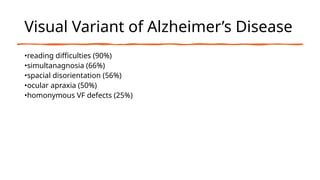
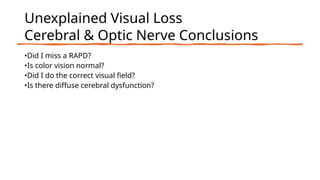
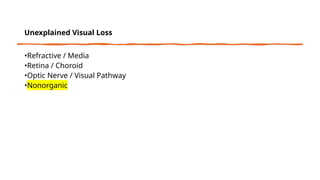
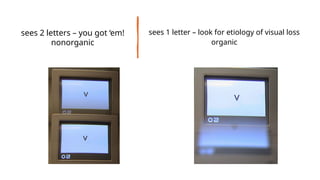







The document discusses the evaluation of patients with unexplained visual loss, outlining potential causes which include refractive, retinal, or optic nerve issues, as well as non-organic factors. It emphasizes the importance of thorough examination and testing methods such as color vision assessment and dark room pupillary responses to differentiate between organic and non-organic visual loss. Additionally, it highlights common misdiagnoses and the need for careful analysis in determining the underlying issues affecting vision.




![Acute visual loss [Compatibility Mode].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/acutevisuallosscompatibilitymode-220808143729-7342aaf9-thumbnail.jpg?width=640&height=640&fit=bounds)











































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)












![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





