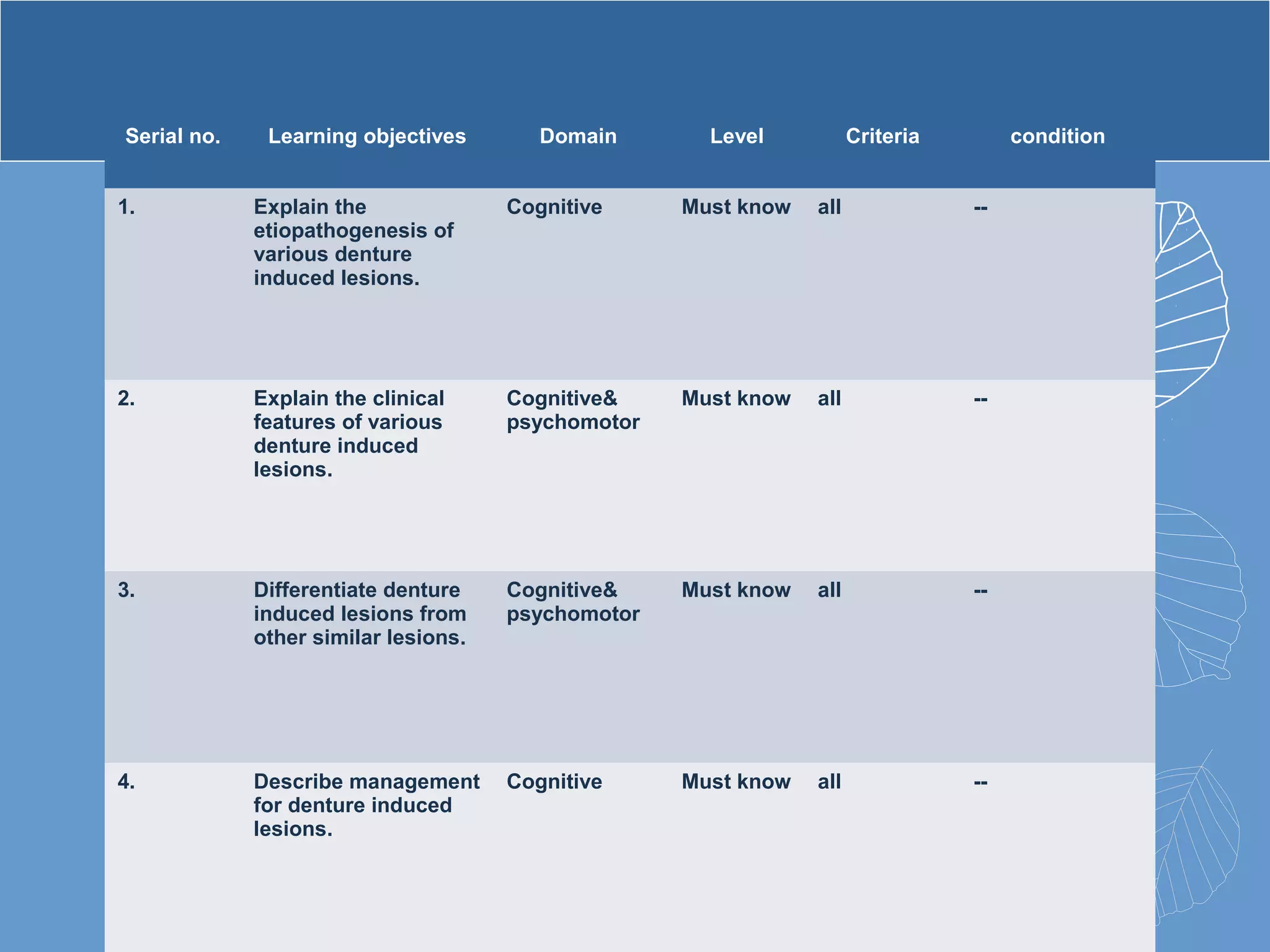
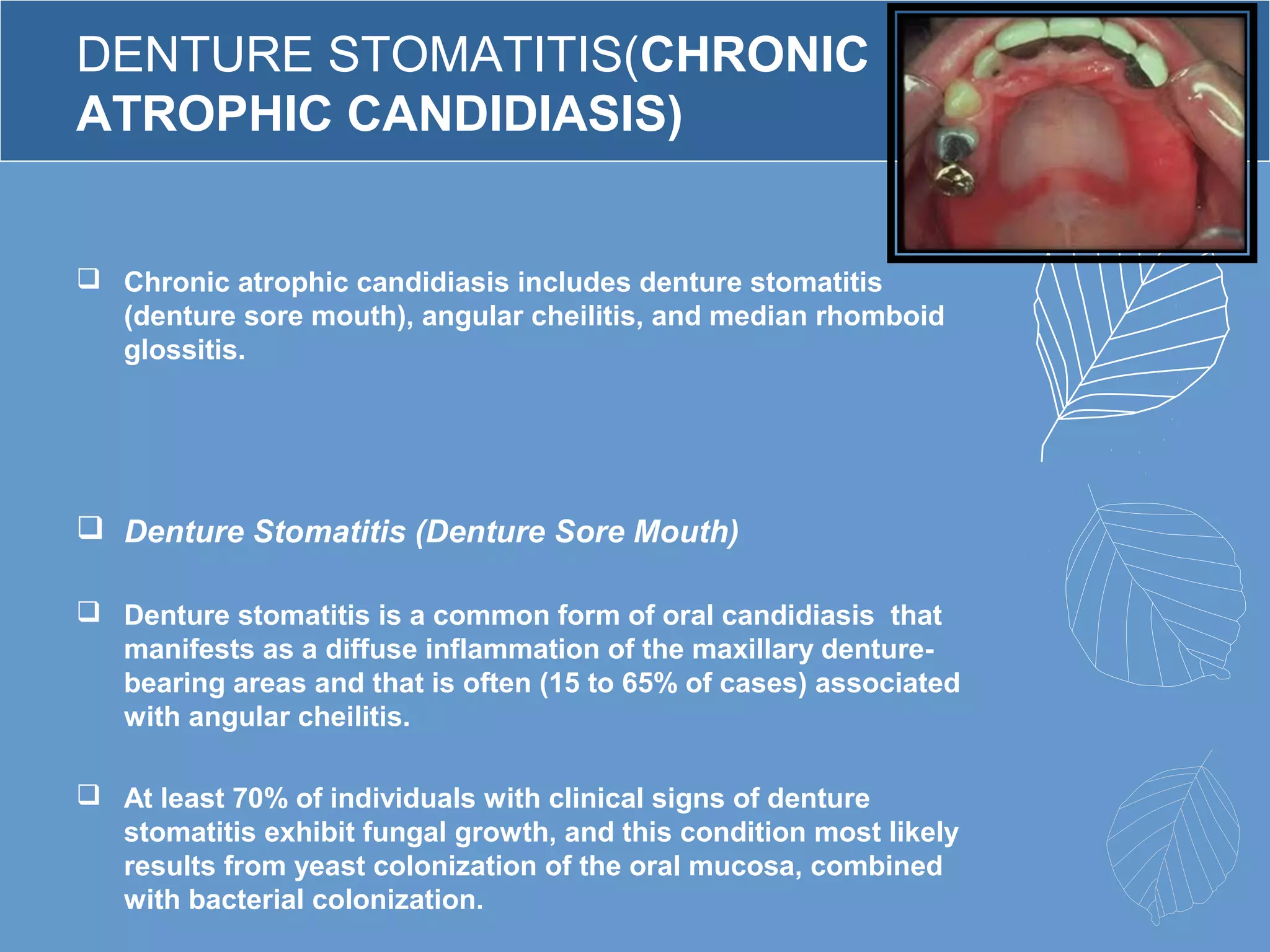
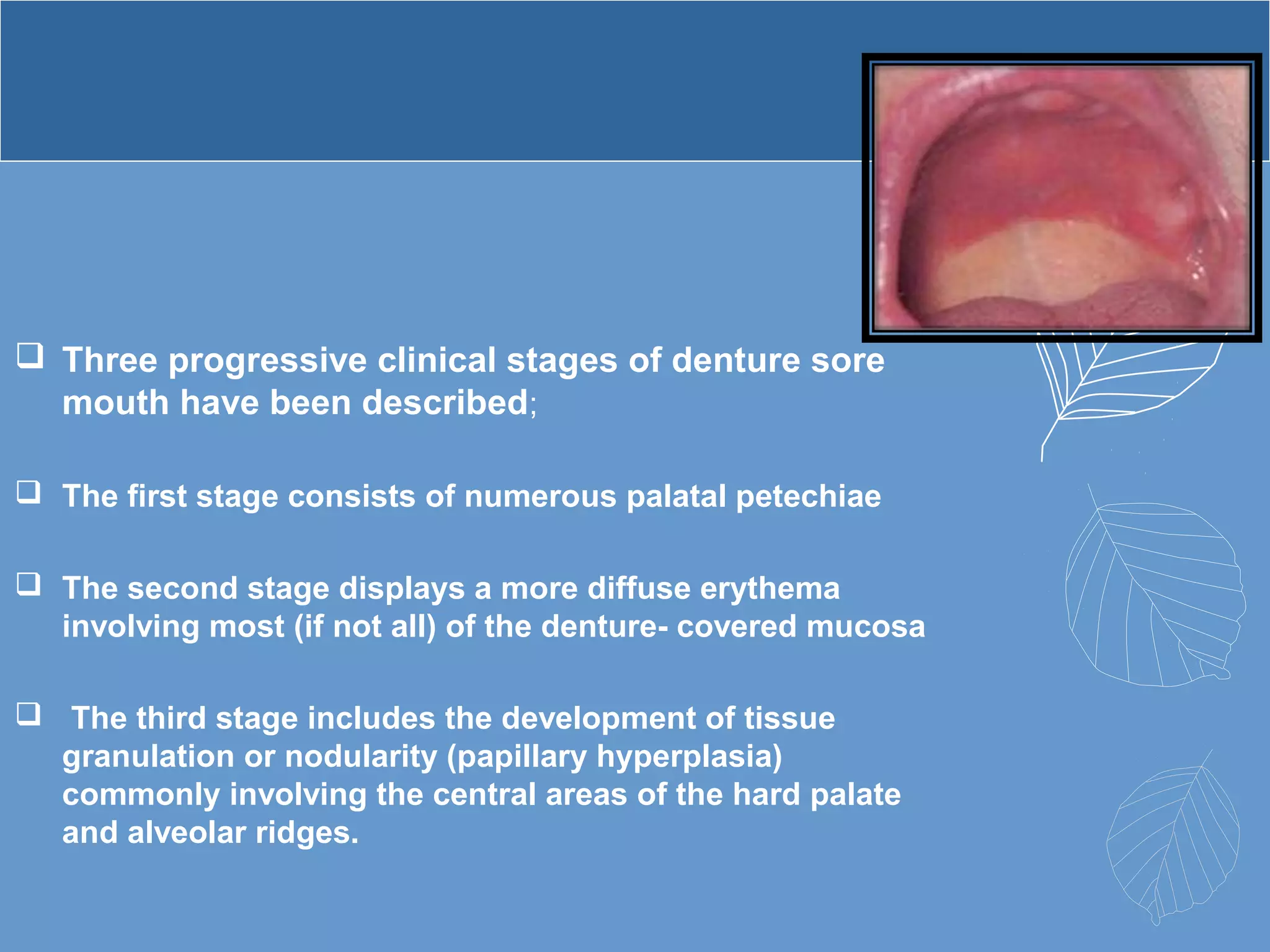
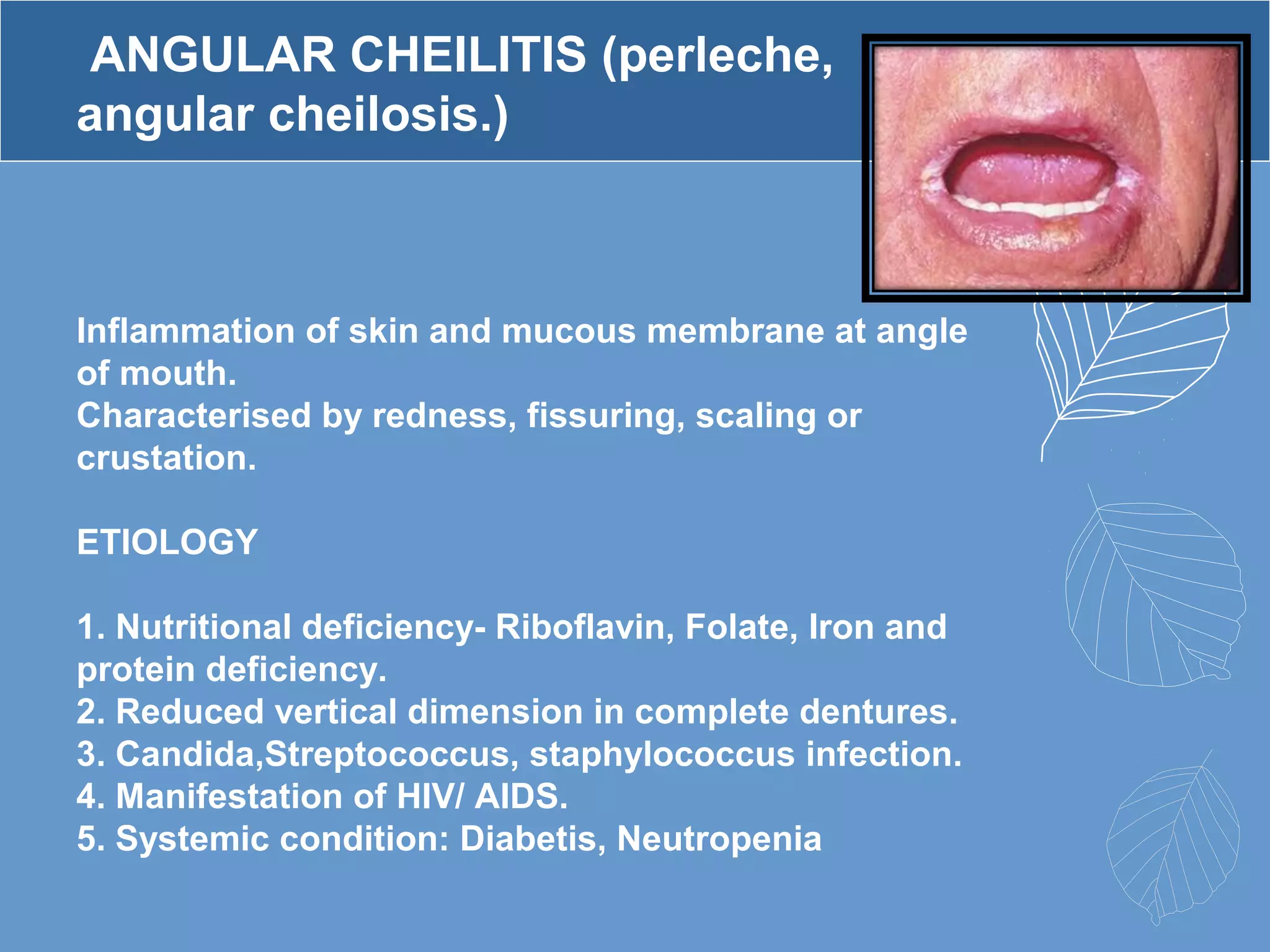
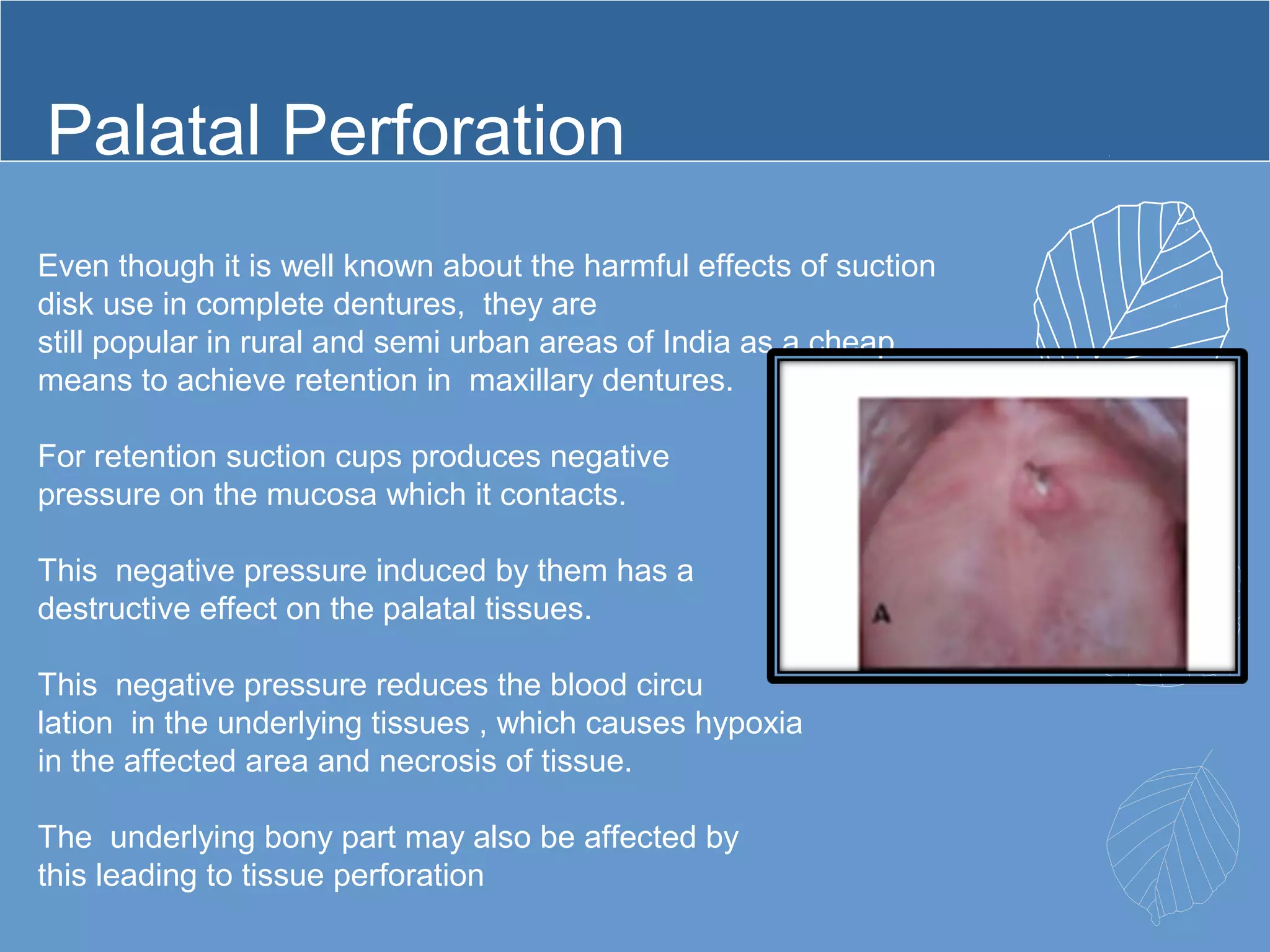
This document provides information about ill-fitting denture induced lesions. It discusses the purpose of the presentation which is to describe the etiology, clinical features, management, and differential diagnosis of various denture induced lesions. It then covers various specific lesions in detail, including traumatic ulcer, cheek bite, inflammatory hyperplasia, fibrous papillary hyperplasia, chronic atrophic candidiasis (denture stomatitis), contact allergy, malignancy, angular cheilitis, and palatal perforation. For each lesion, it discusses causes, clinical features, and management.