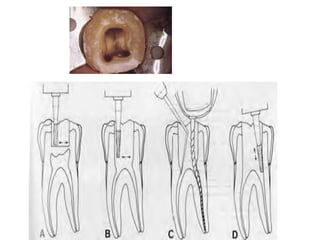
![Access
openings
are
made
preferably
with
High
speed
instruments.
The bur should start rotating before touching the tooth surface
and should continue rotating even after you take it out of the
cavity.
There should be good illumination [and magnification]
Once the roof of the chamber is opened, canals are located with
the endodontic probe](https://image.slidesharecdn.com/accesscavitypreparation-140121154007-phpapp01/85/Access-cavity-preparation-7-320.jpg)

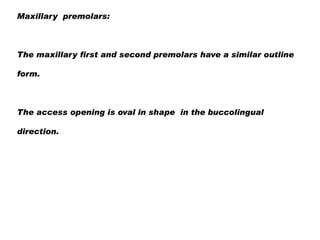
![Maxillary second Premolar
It usually has one root and one canal in 53-60%
The access opening is similar to the first premolar but it
does not have the bucco lingual extension as much as
the first premolar.
[unless if it has two canals]](https://image.slidesharecdn.com/accesscavitypreparation-140121154007-phpapp01/85/Access-cavity-preparation-21-320.jpg)
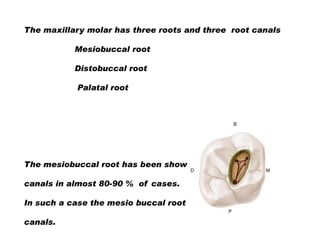



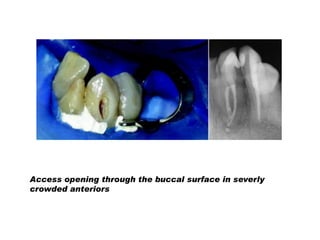
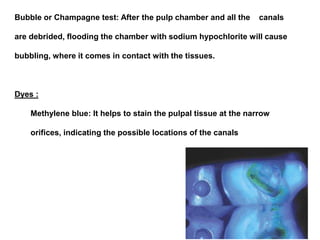
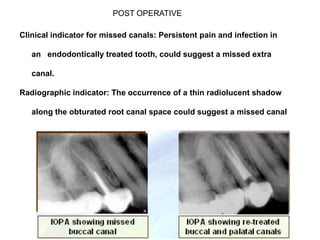

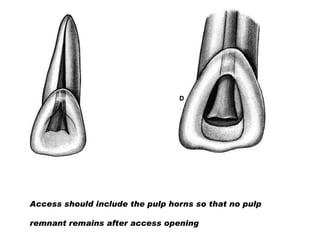
This document provides guidance on accessing tooth canals during root canal treatment. It discusses locating all canals, removing pulp tissue while conserving tooth structure. Access openings should be made under rubber dam isolation using high-speed instruments with good illumination. Tooth anatomy and pre-operative x-rays are used to determine the number and location of canals. Care must be taken to locate extra canals which may be present, especially in teeth with complex anatomy.









































































