The document discusses pupil function and abnormal pupil reactions. It covers:
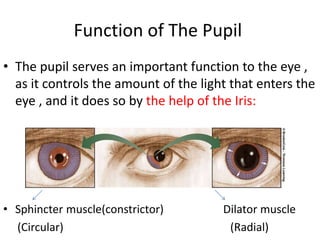
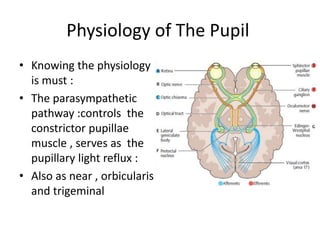
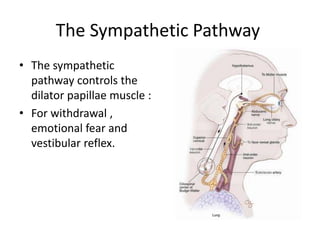
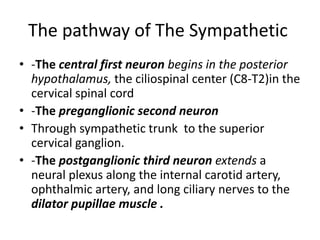
1. The physiology of pupil constriction and dilation which is controlled by the parasympathetic and sympathetic nervous systems respectively.
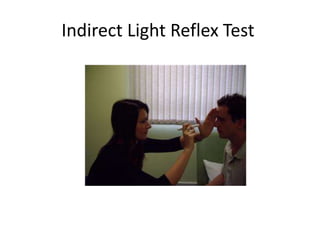
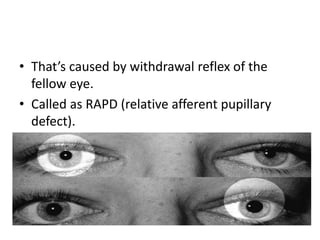
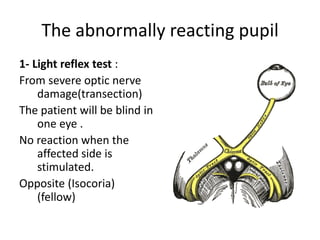
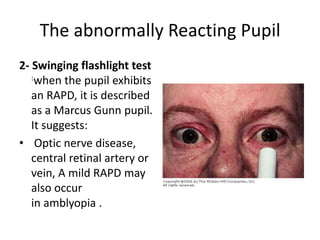
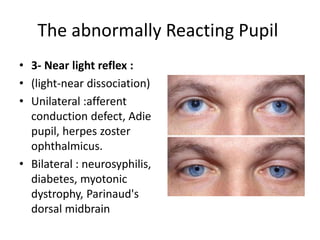
2. How to examine pupils including observing size and shape, light reflex testing, swinging flashlight test, and near reflex testing.
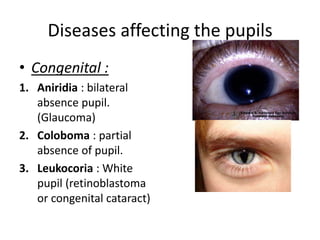
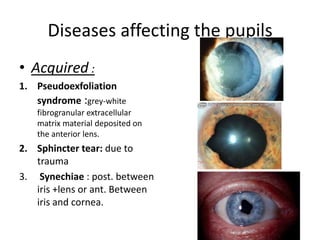
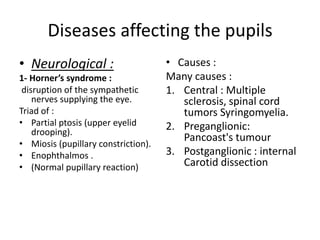
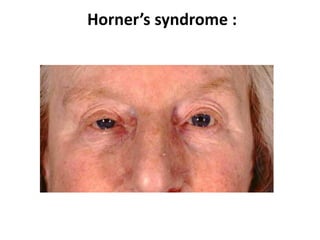
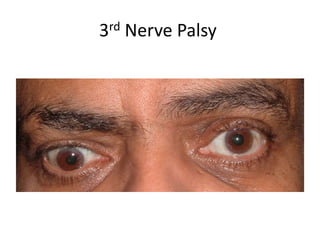
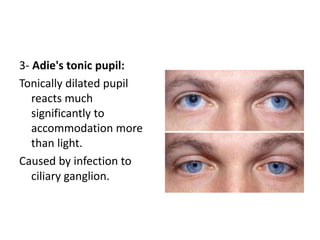
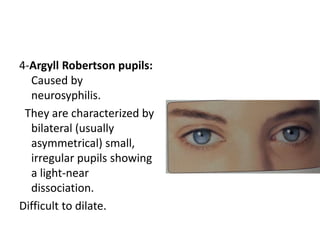
3. Various diseases and conditions that can cause abnormal pupil reactions like Horner's syndrome, third nerve palsy, Adie's tonic pupil, and Argyll Robertson pupils.
4. Drugs that can cause mydriasis or miosis by affecting the parasympathetic or sympathetic pathways.