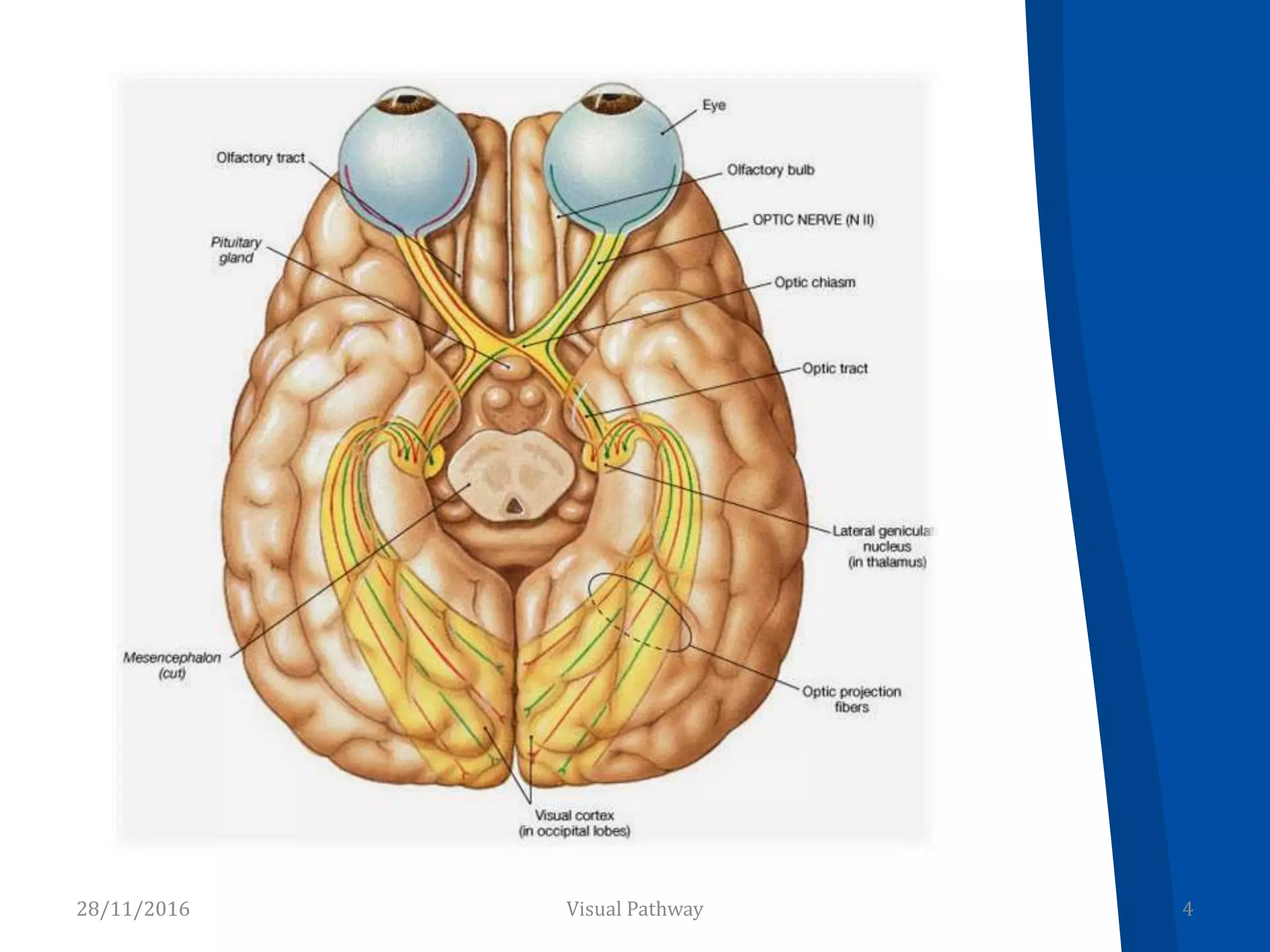
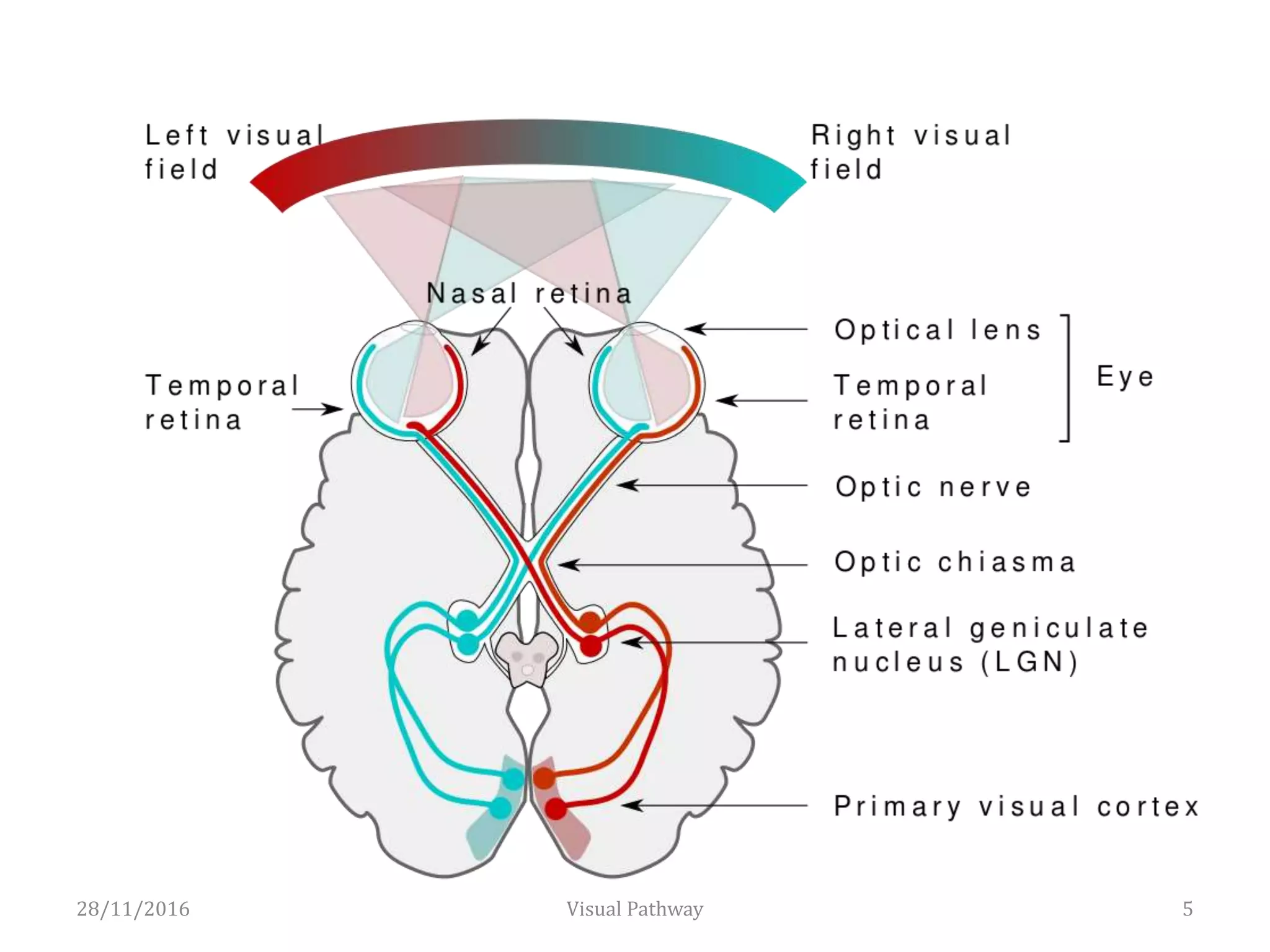
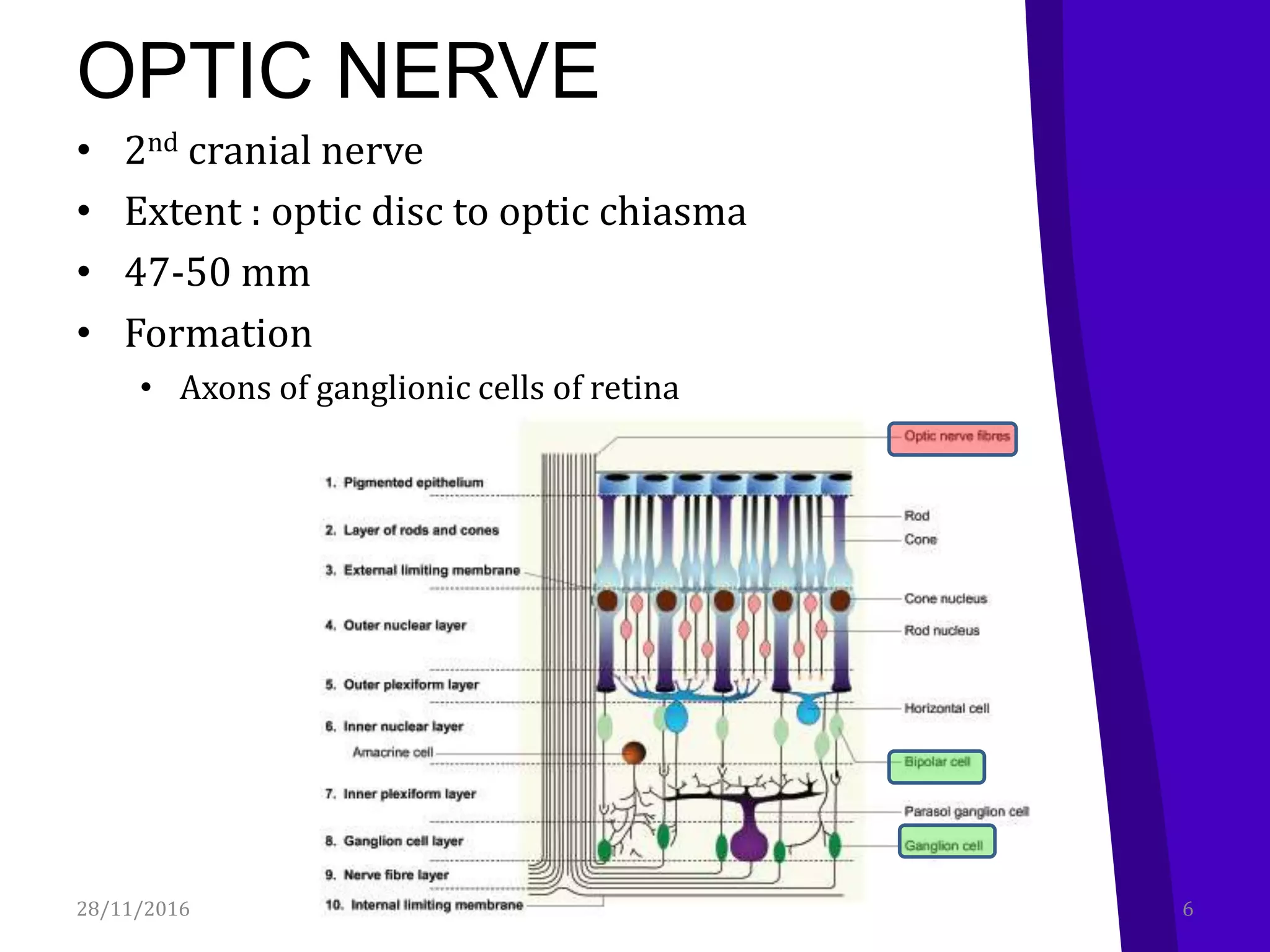
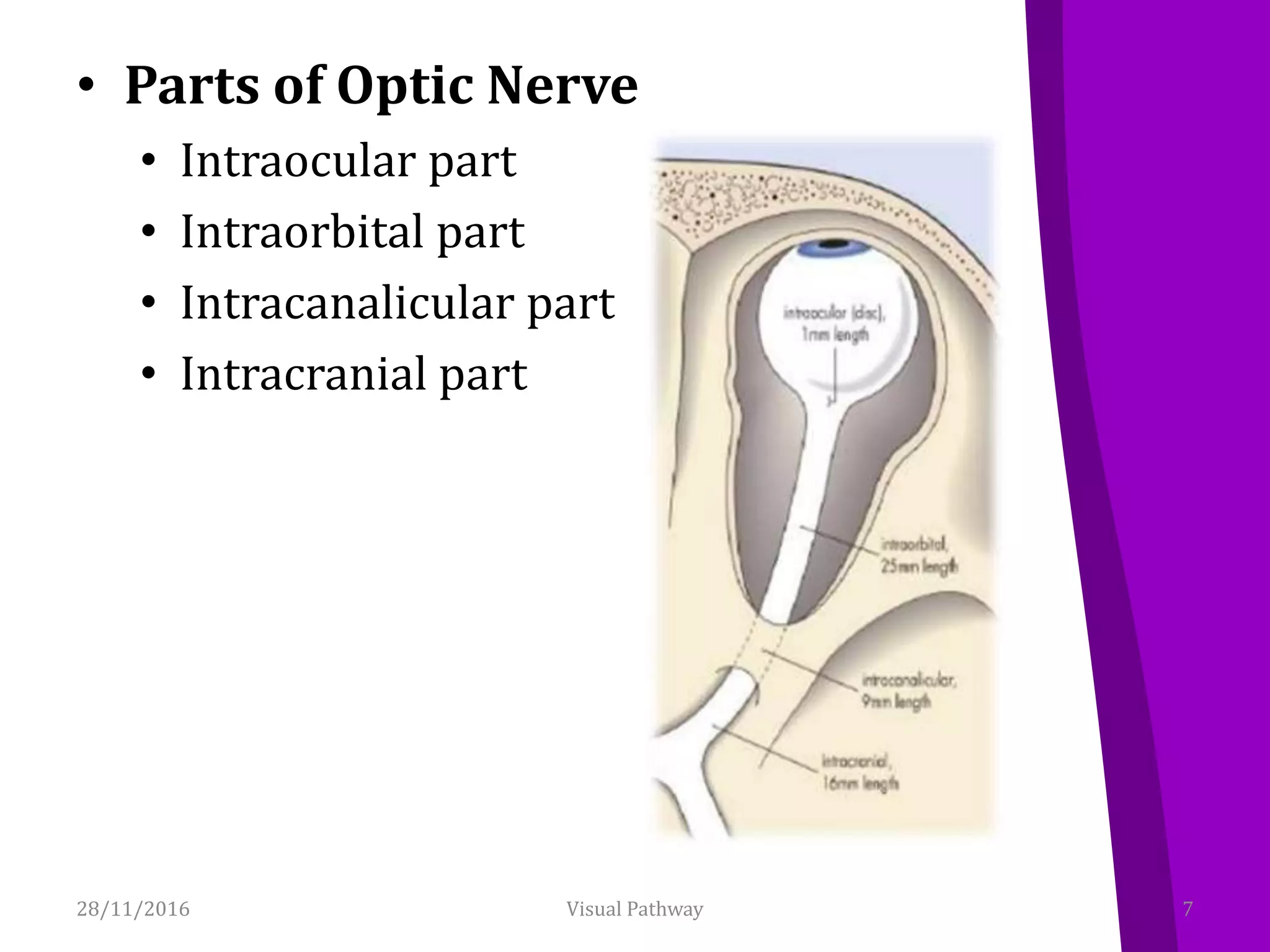
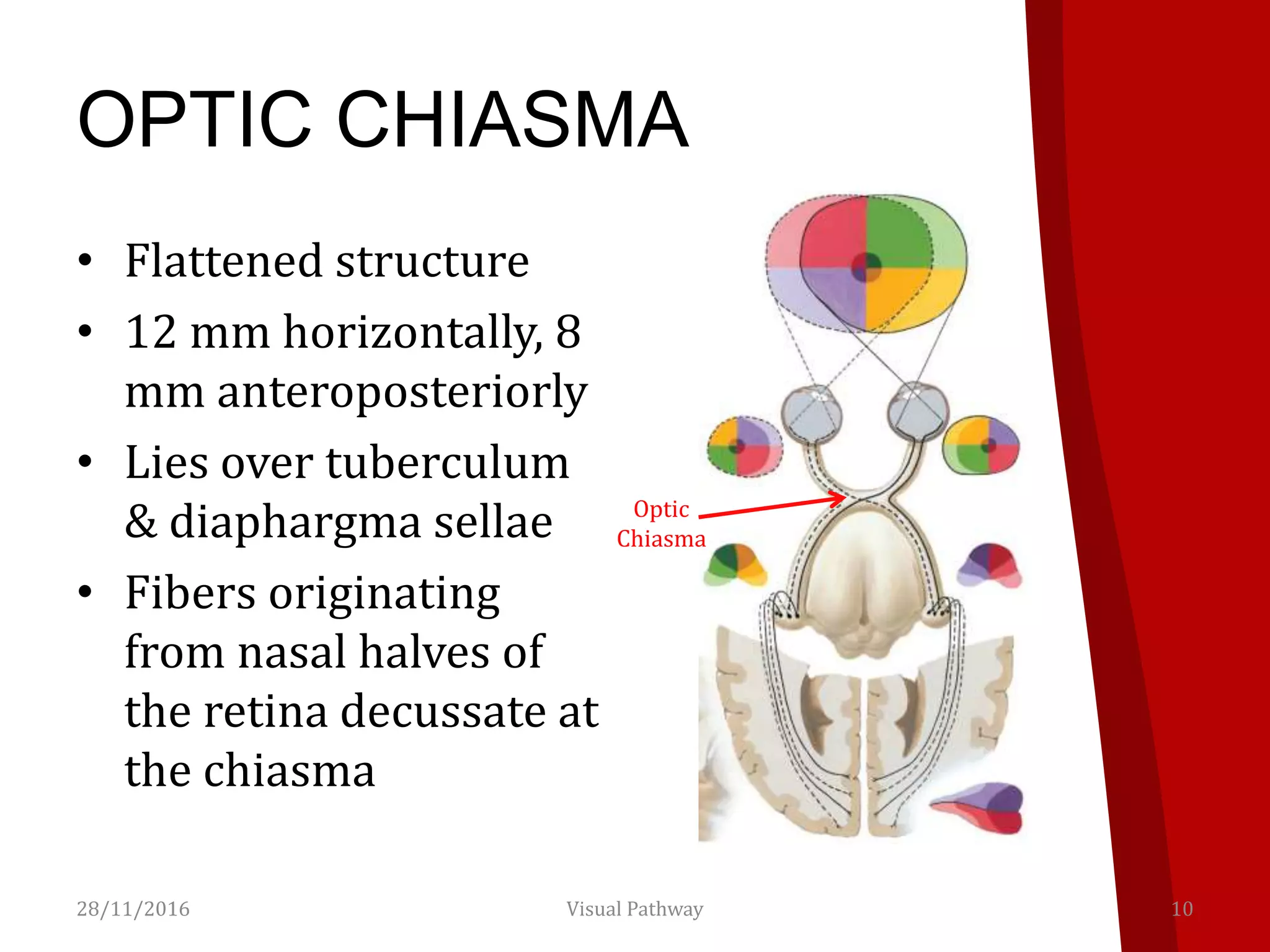
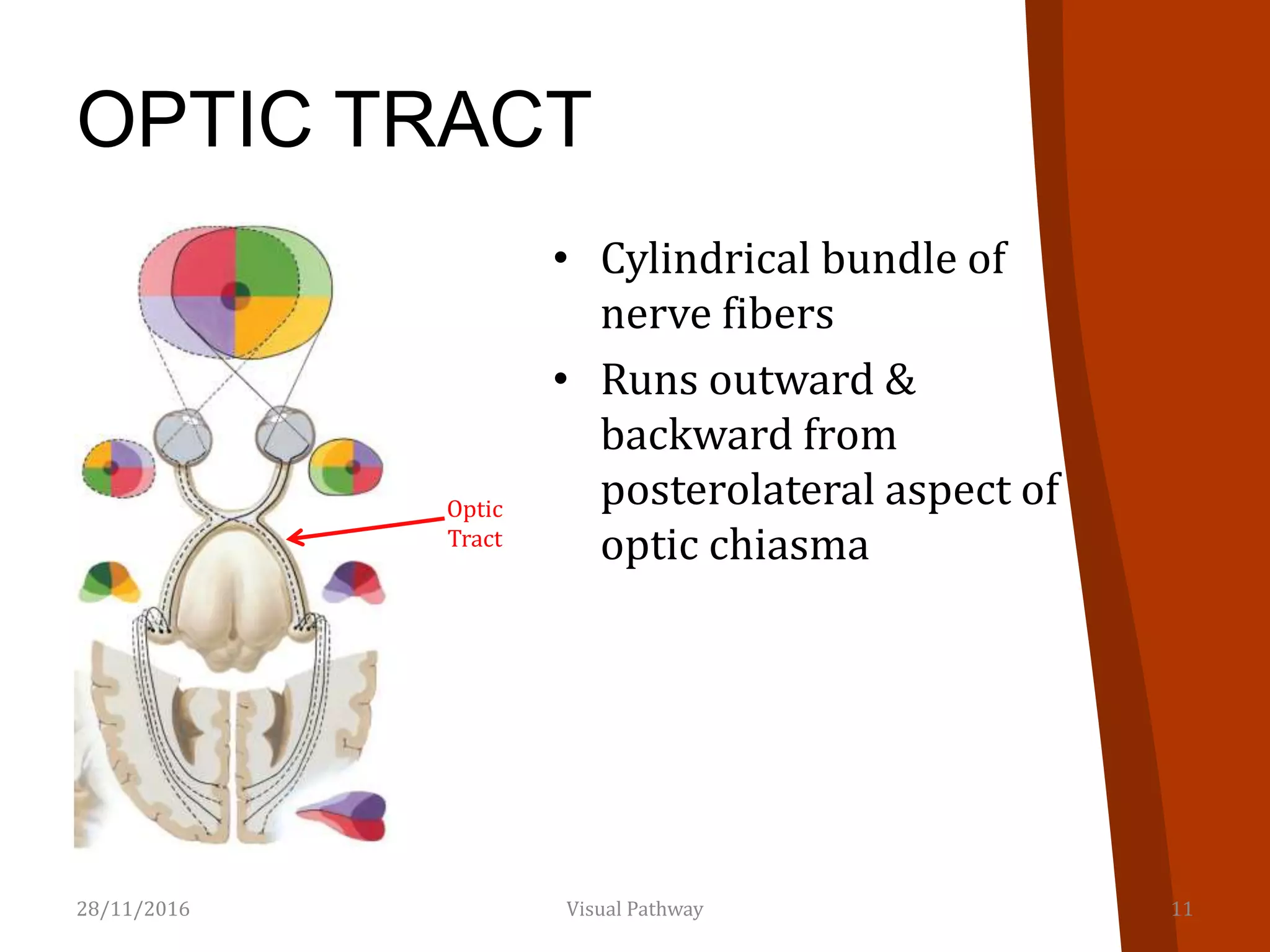
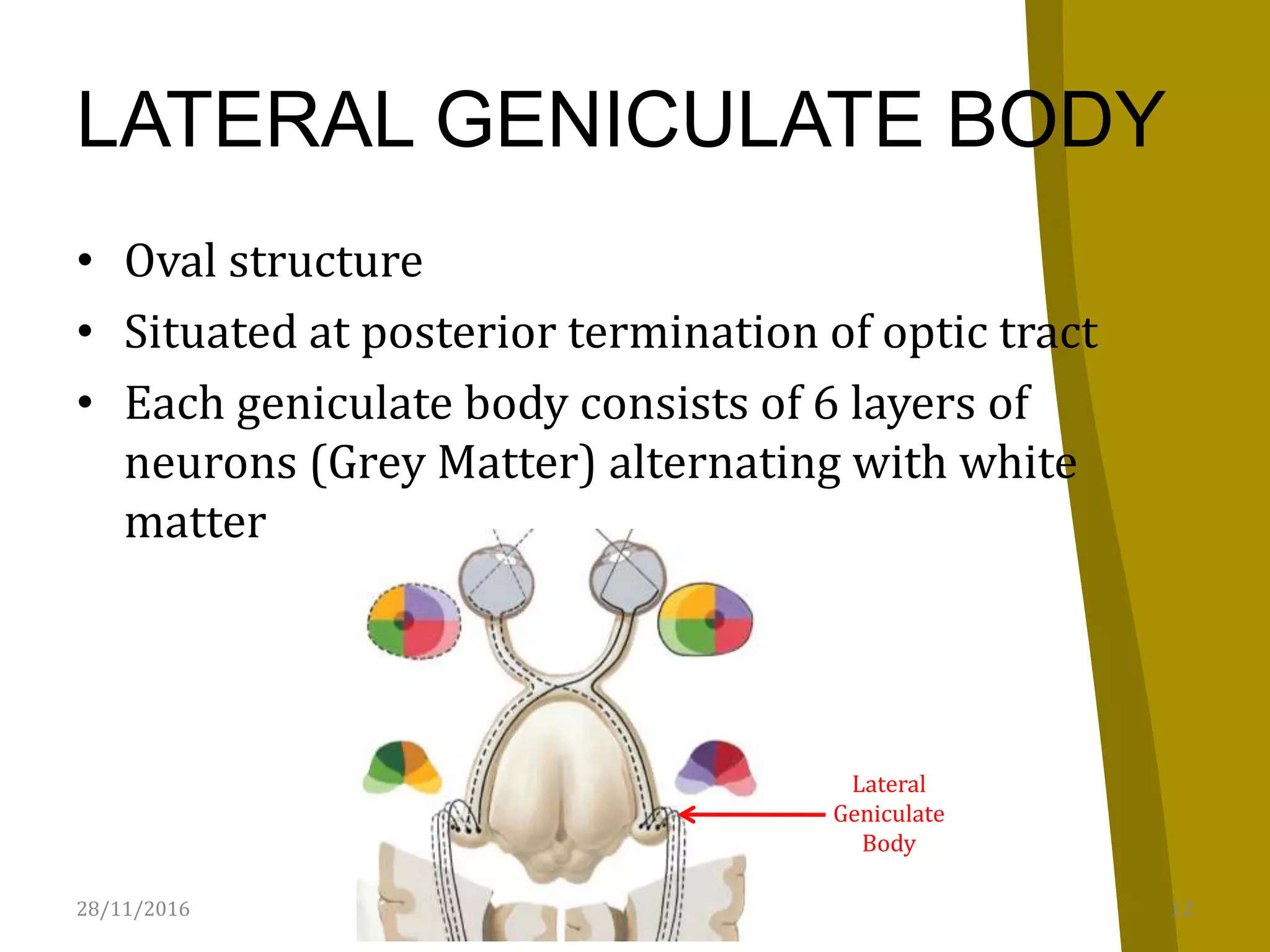
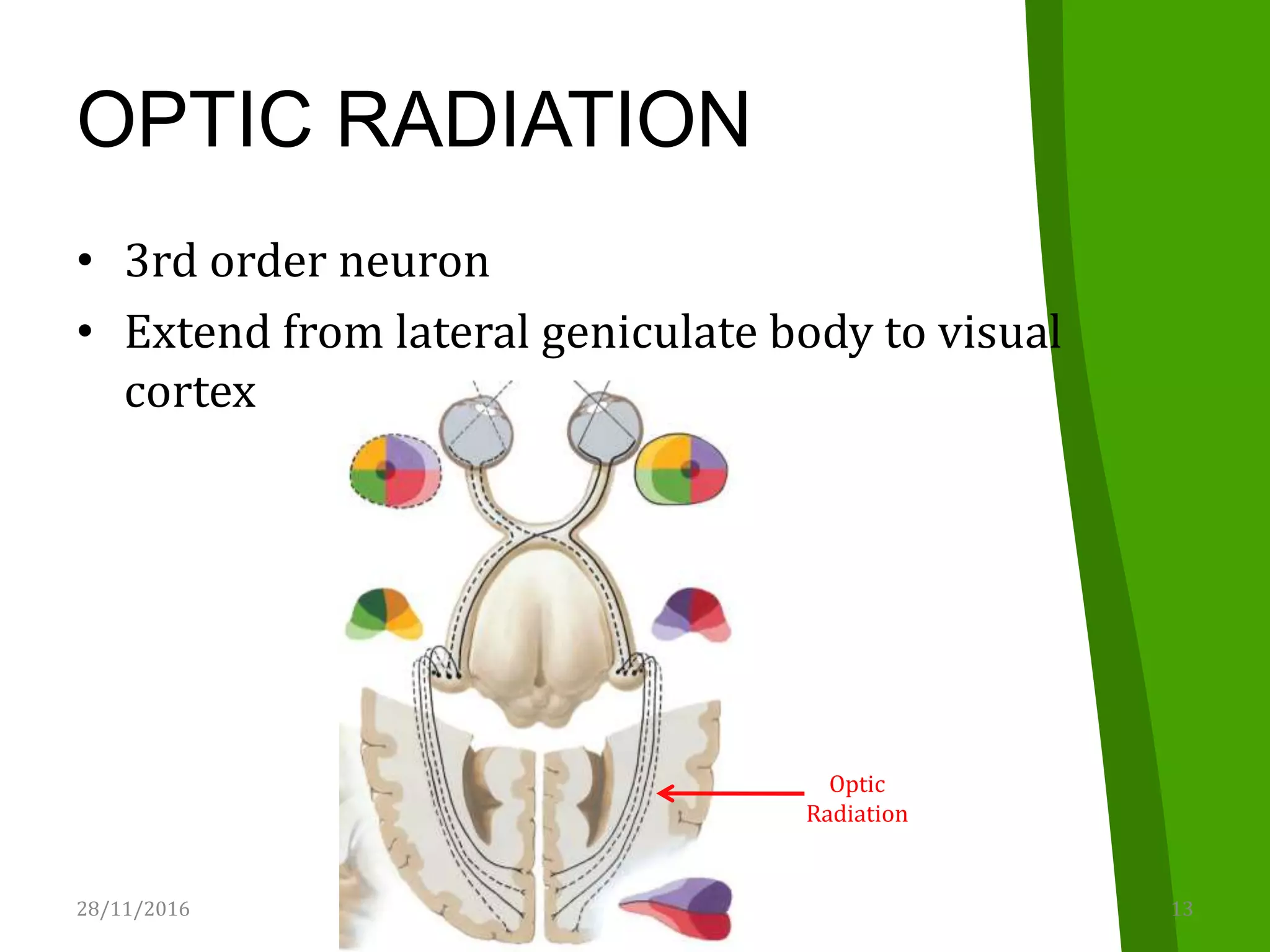
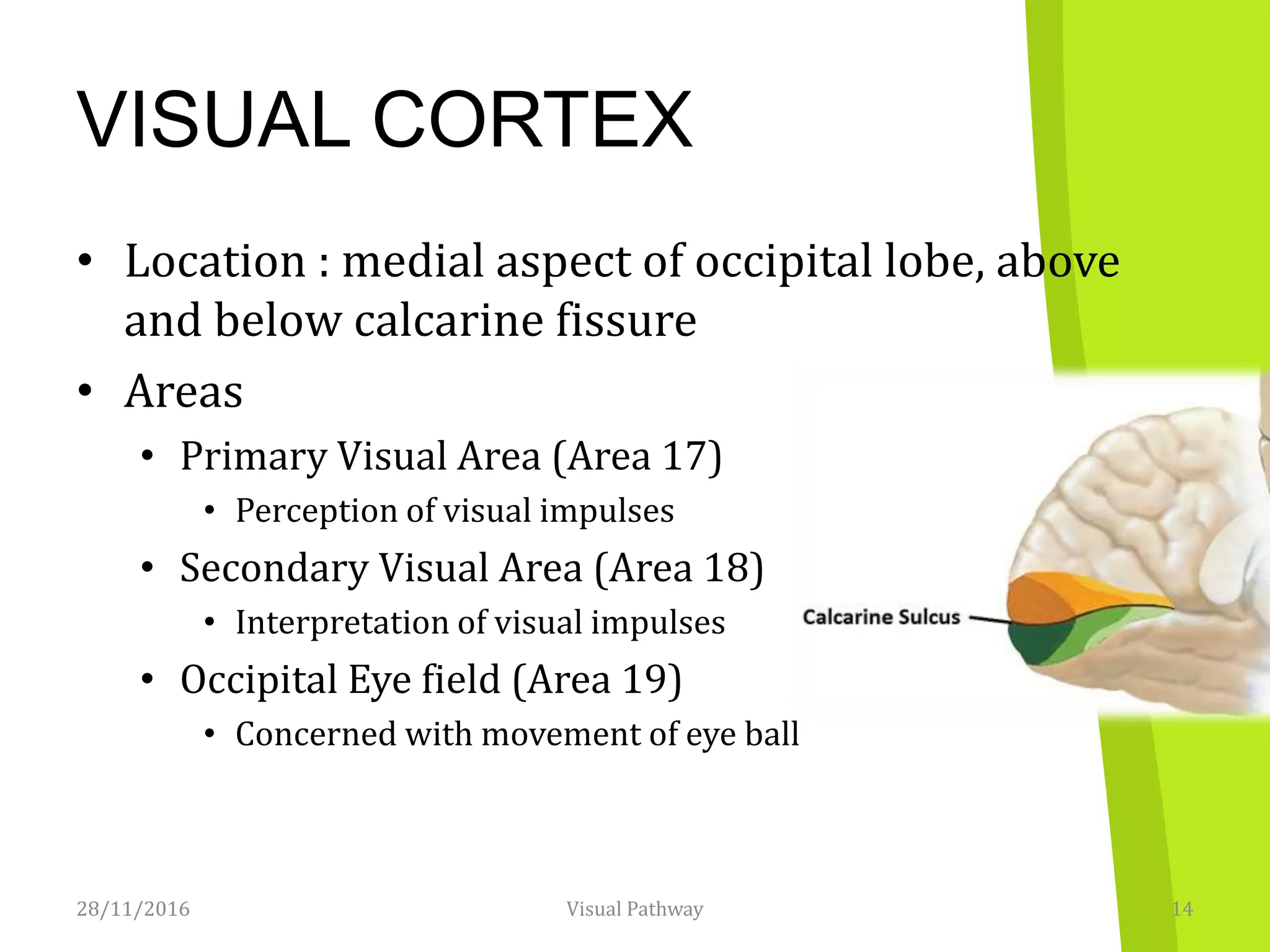
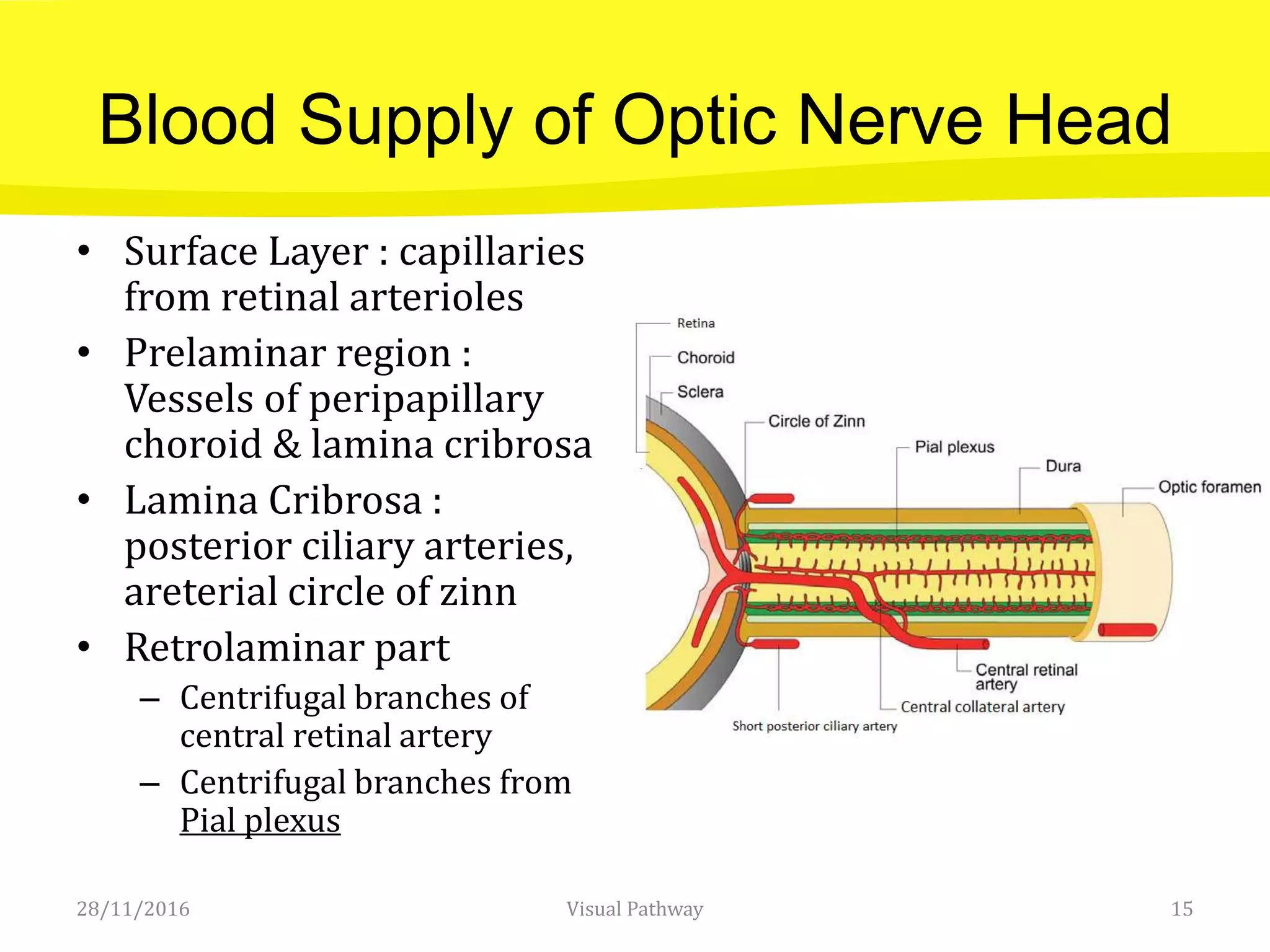
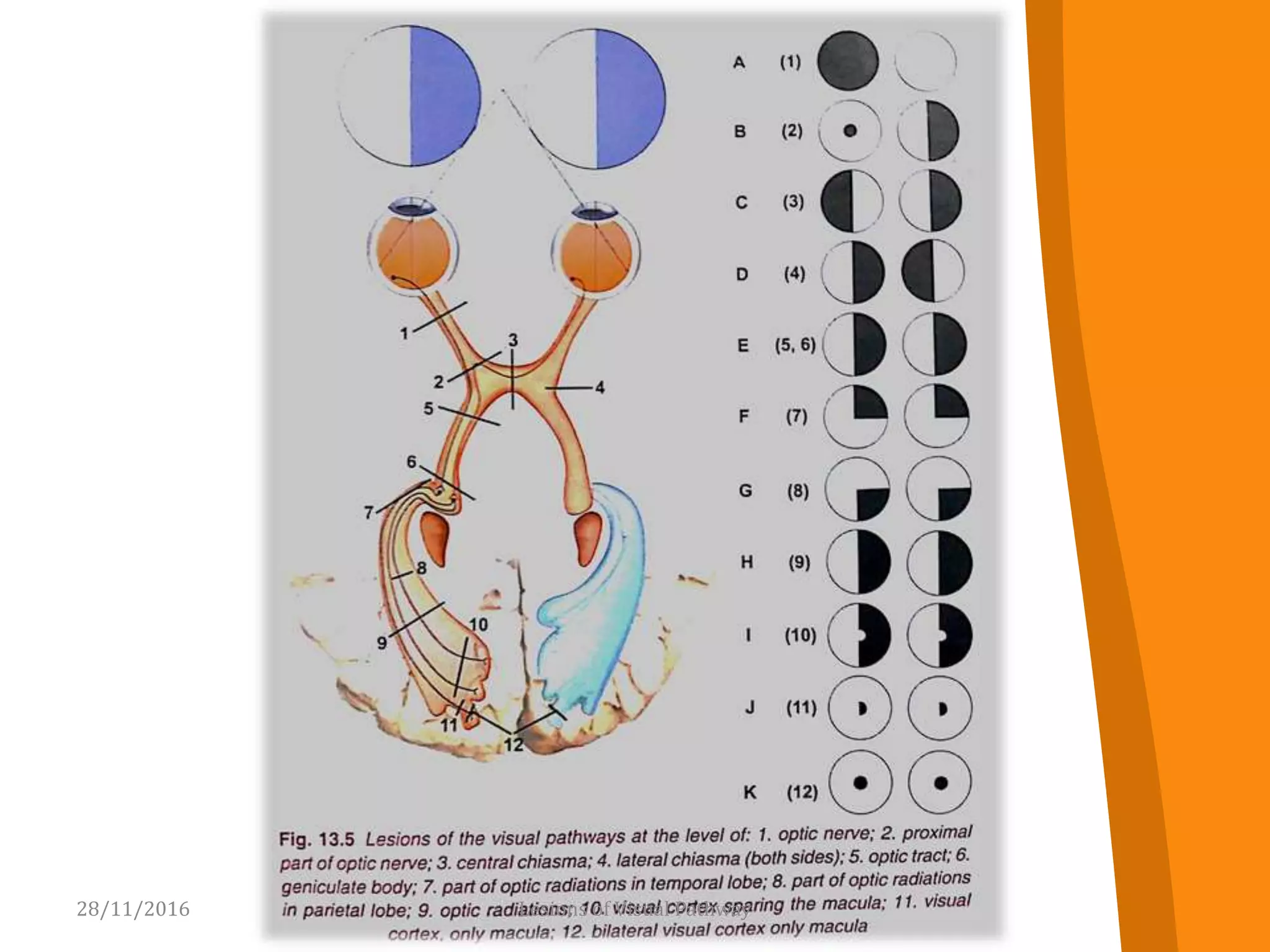
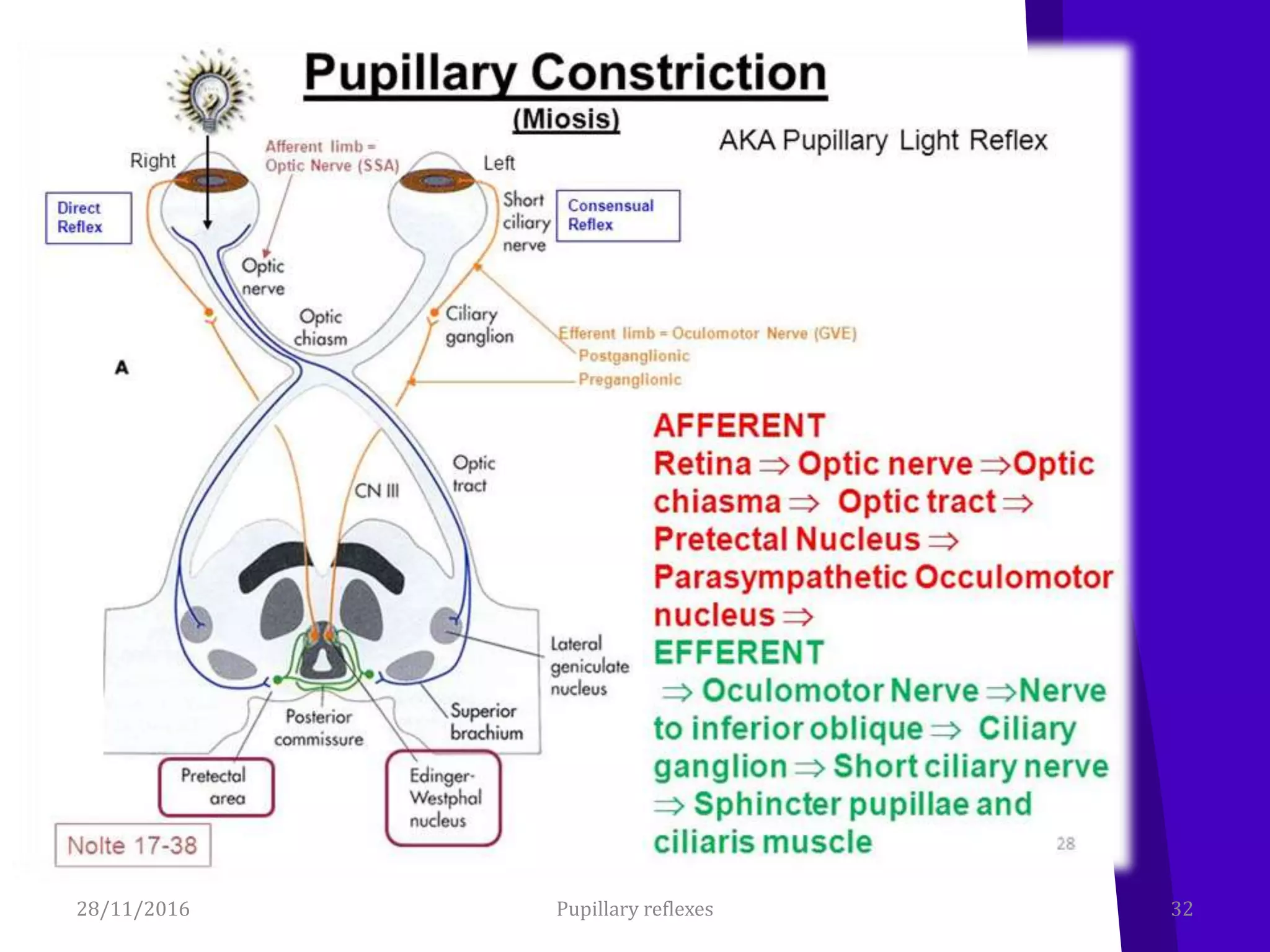
The document provides an overview of the visual pathway, including its anatomy and physiology. It describes the main components of the visual pathway - the optic nerve, optic chiasm, optic tracts, lateral geniculate bodies, optic radiations, and visual cortex. It then discusses lesions that can occur along the visual pathway and their associated signs and symptoms. Finally, it covers pupillary reflexes like the light reflex and near reflex, as well as abnormalities in pupillary reactions.