Downloaded 135 times


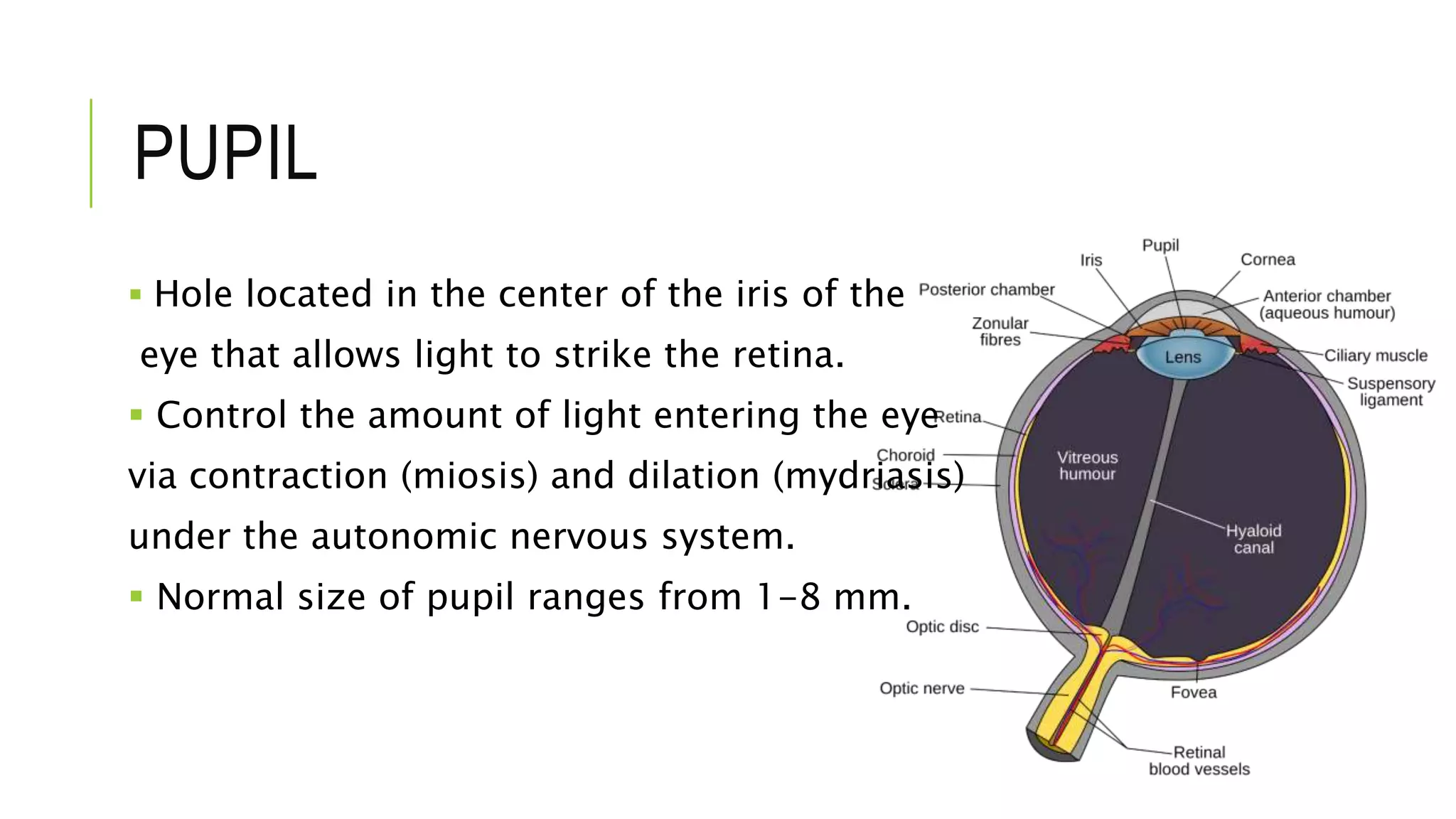


















1. The document discusses the pupil, normal pupil reactions, and various abnormalities of the pupil. 2. It describes tests like direct light response, swinging flashlight, and accommodation response that are used to assess the pupil. 3. Abnormalities are categorized based on whether they cause isocoria (equal pupil size) or anisocoria (unequal pupil size). Disorders causing isocoria include Argyll Robertson Pupil and Parinaud Oculoglandular Syndrome. Disorders causing anisocoria include Complete Oculomotor Palsy, Tonic Pupil, and Horner Syndrome.


























































































