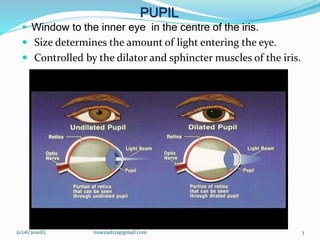
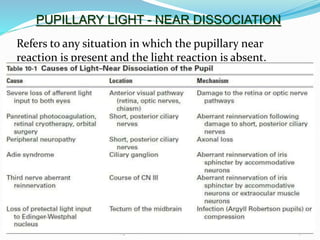
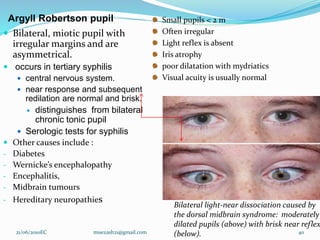
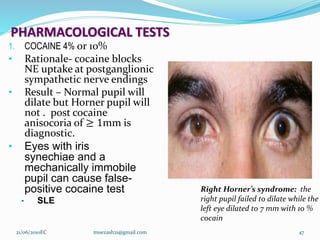
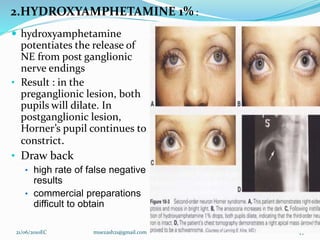
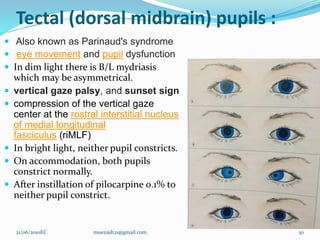
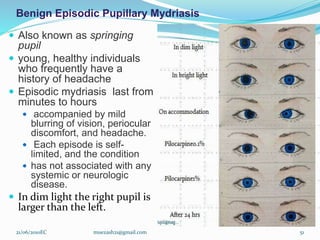
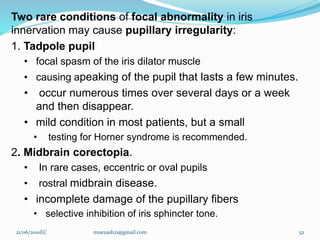
This document discusses pupillary abnormalities and tests. It begins with an overview of pupillary anatomy and functions. It describes features of the normal pupil and various abnormalities including anisocoria. It discusses defects in the afferent pathway such as total and relative afferent pathway defects. Efferent pathway defects and causes like Horner's syndrome and Adie's tonic pupil are explained. The document concludes with a discussion of pharmacological tests used to evaluate pupillary abnormalities.