Downloaded 208 times
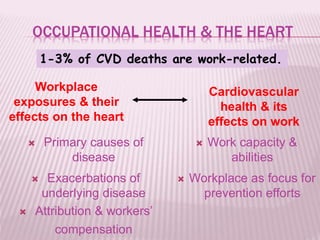
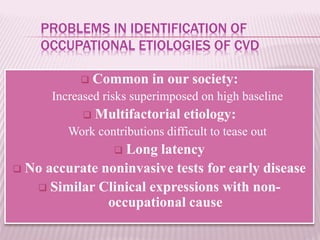
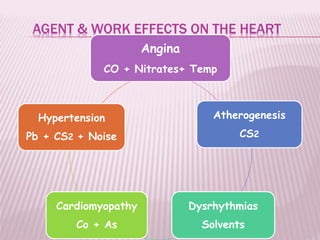
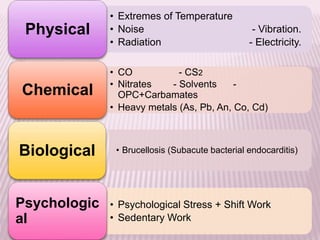



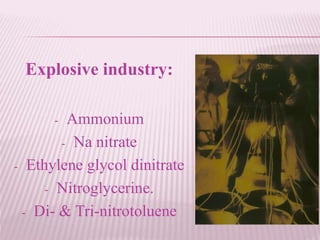
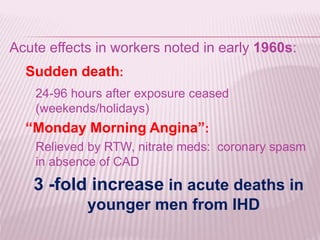
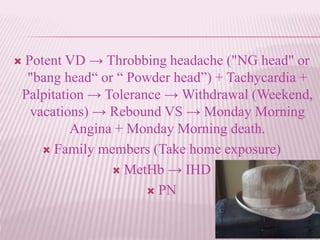
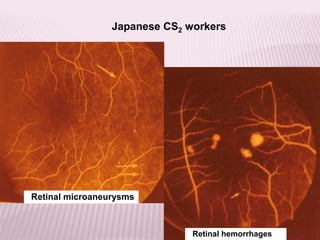
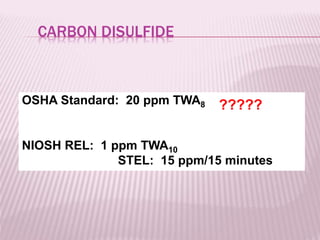
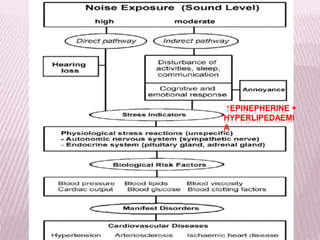



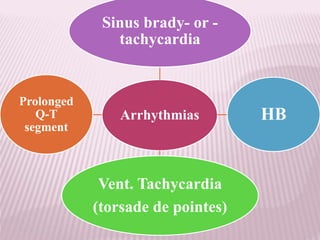
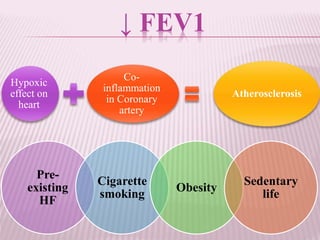
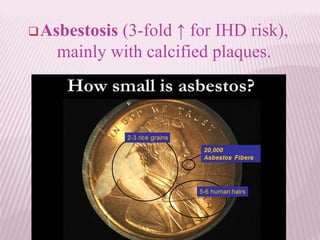

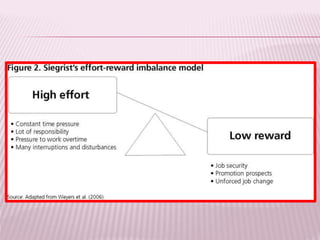
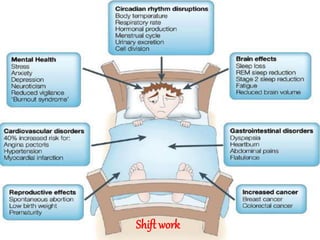
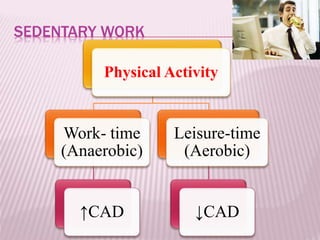


The document discusses occupational heart diseases, detailing various workplace exposures that can adversely affect cardiovascular health, including chemicals like carbon monoxide and carbon disulfide, as well as stress from high job demands. It highlights the difficulty in identifying occupational causes of cardiovascular diseases, the multifactorial nature of these conditions, and associated risks for various workforces. Recommendations include the need for improved monitoring and preventive strategies in workplaces to mitigate these health risks.











































































































