Downloaded 119 times

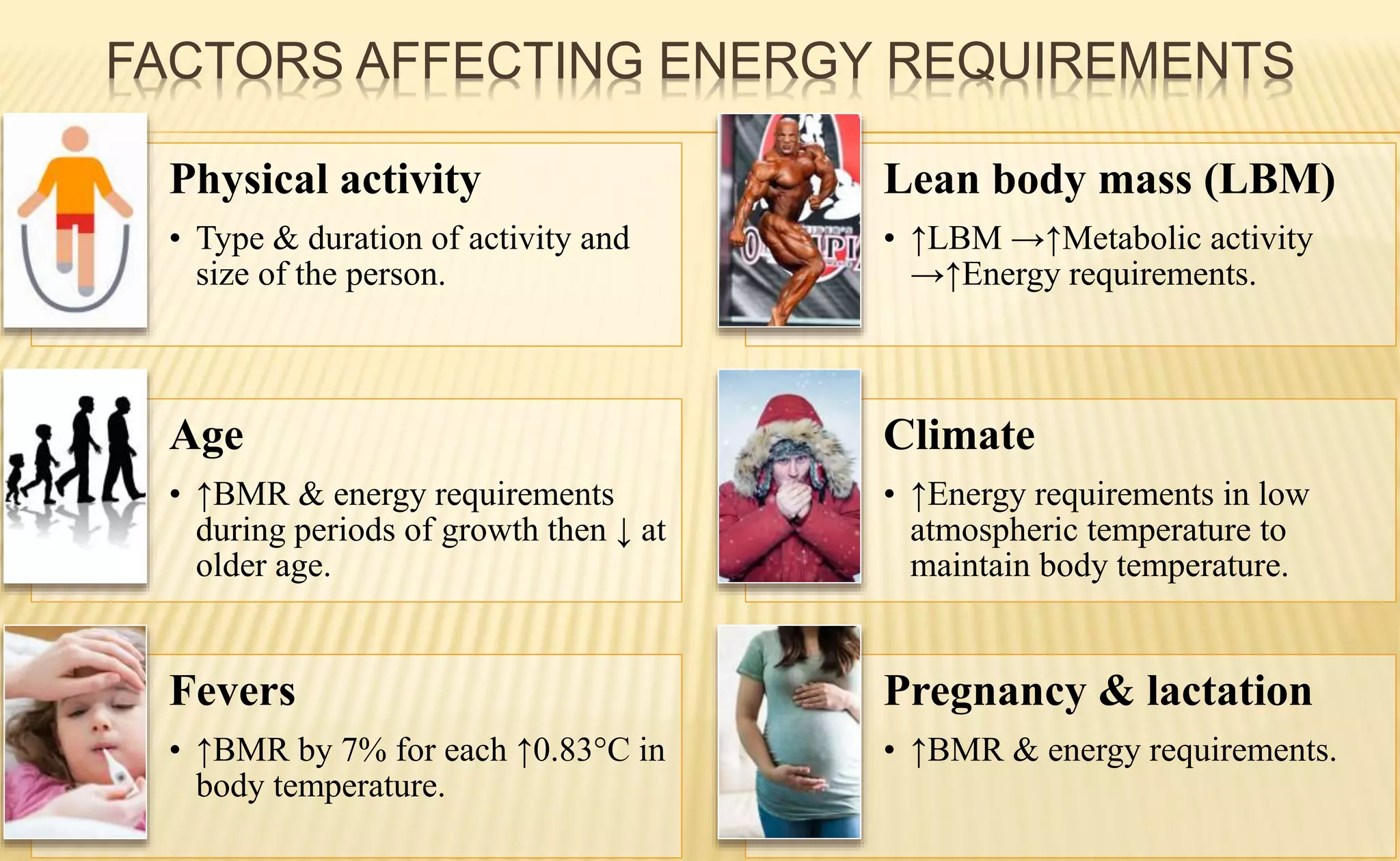













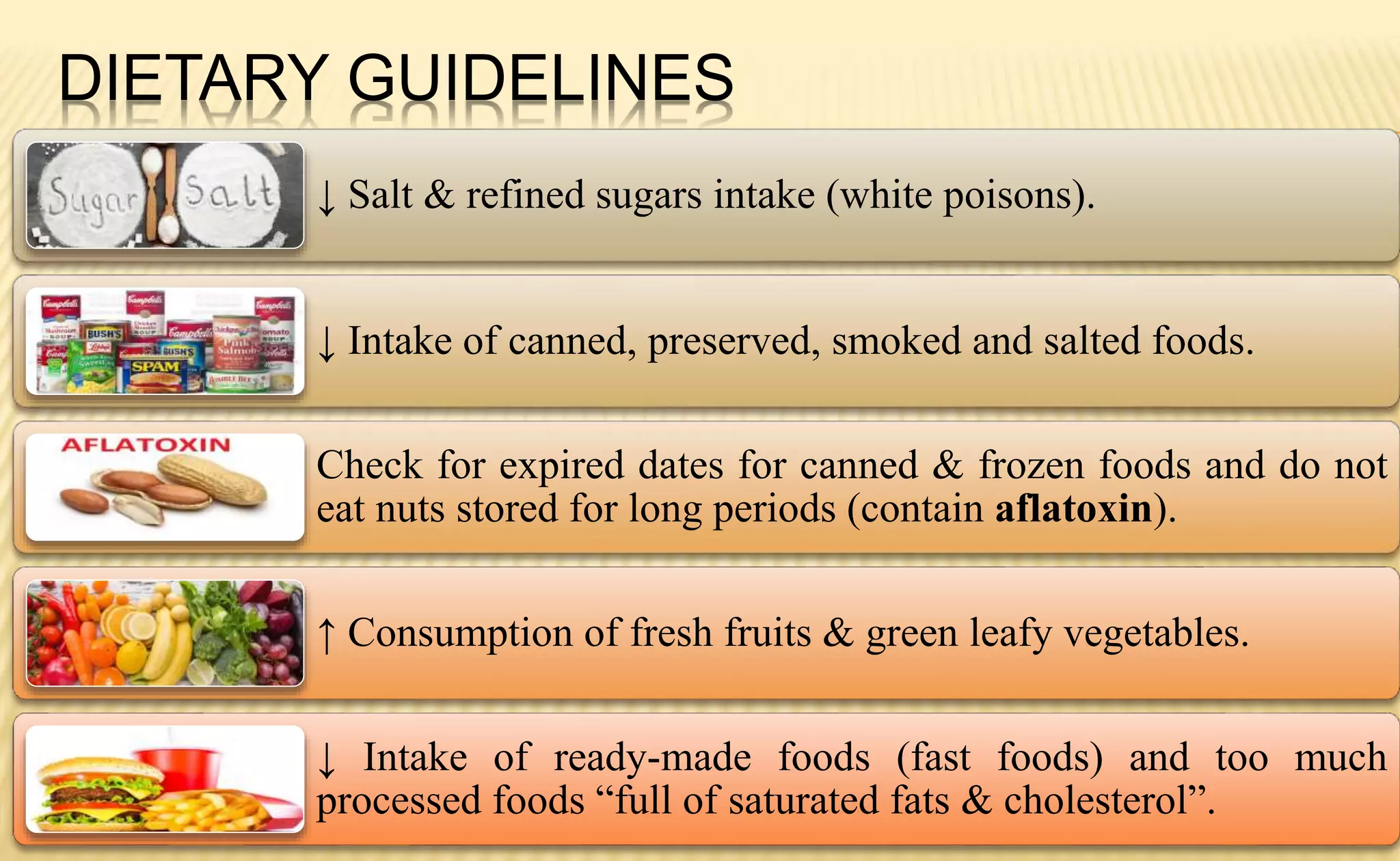

















































The document outlines essential learning objectives related to nutrition, including the identification of nutrient sources, functions, and the effects of deficiencies, as well as the development of diet plans for various vulnerable groups. It details factors affecting energy requirements, the significance of the glycemic index, and provides dietary guidelines. Furthermore, it highlights the nutritional needs of different demographic groups and methods for assessing nutritional status through various evaluation techniques.























































































