Downloaded 135 times


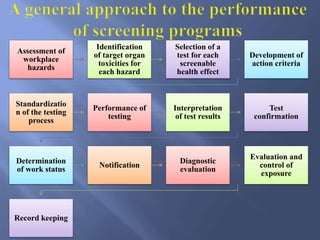
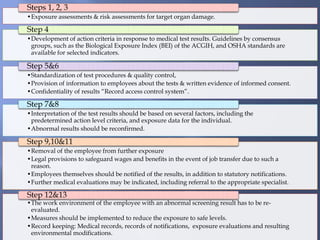
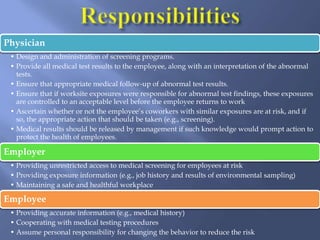
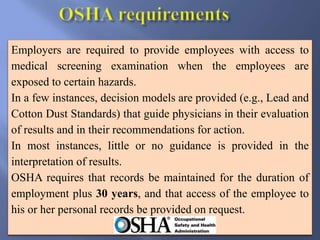
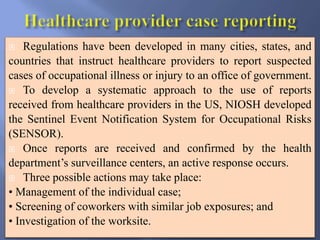

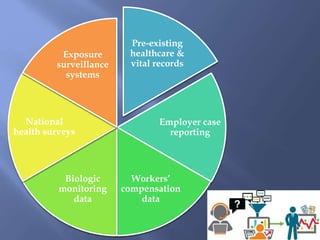
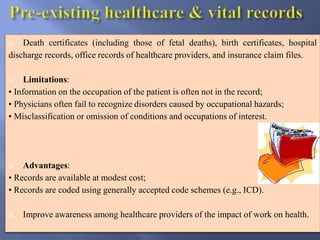
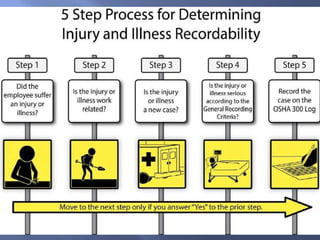
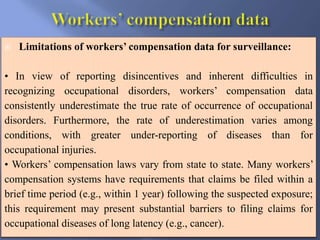



The document details the components and processes of occupational health surveillance, emphasizing the importance of systematic data collection, analysis, and interpretation for public health practice. It outlines the roles of healthcare providers, employers, and employees in ensuring workplace safety through screening, exposure assessments, and legal obligations for reporting occupational illnesses. Additionally, it discusses limitations and advantages of various data sources for monitoring occupational disorders, including workers' compensation and health surveys.




















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


