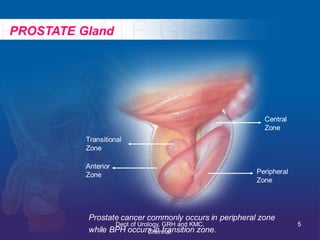
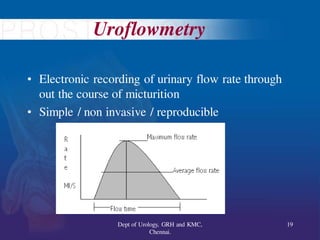
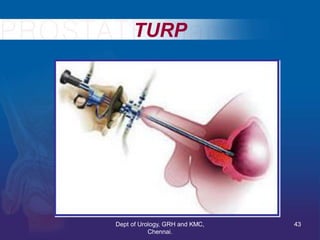
This document provides information on benign prostatic hyperplasia (BPH) and its management. It discusses the anatomy and histology of the prostate gland, the pathophysiology of BPH, evaluation and diagnostic testing for BPH including digital rectal exam, PSA, uroflowmetry, post-void residual measurement, and pressure flow studies. Symptom scoring and quality of life assessments for BPH are also reviewed. The document outlines the management options for BPH including watchful waiting, medical therapy with alpha blockers and 5-alpha reductase inhibitors, and surgical therapies such as transurethral resection of the prostate, open prostatectomy, and minimally invasive procedures including transurethral incision of









































































![Benign Prostatic Hyperplasia BPH [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/bphedmond-140716213908-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)







![Urinary Diversion after cystectomy [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/urinarydiversionedmond-140716212817-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)









































































