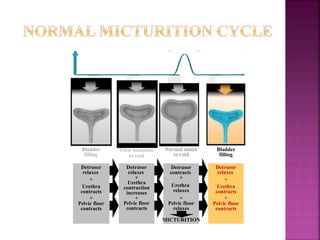
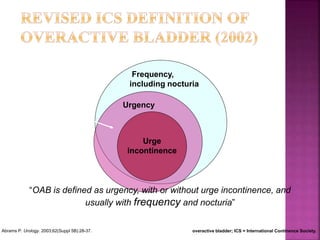
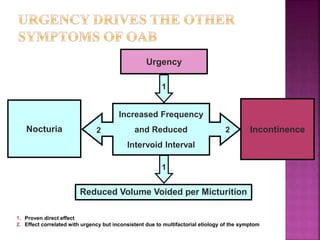
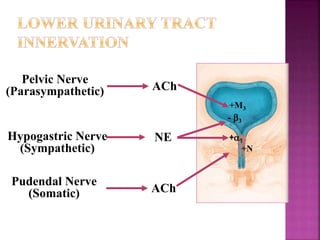
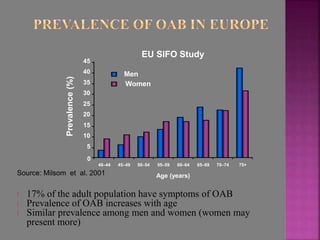
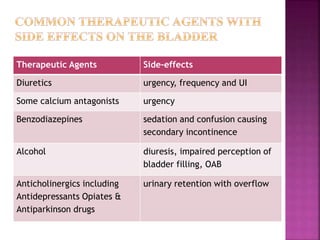
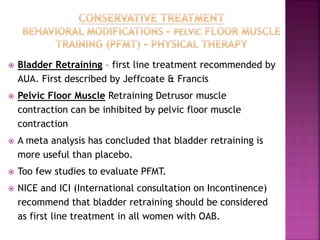
The document discusses overactive bladder (OAB), characterized by symptoms such as urgency, urge incontinence, frequency, and nocturia, emphasizing its multifactorial etiology and pathophysiological mechanisms. It outlines the clinical diagnosis, assessment methods, and various treatment options including bladder retraining and the use of botulinum toxin. The prevalence of OAB is significant, especially in older populations, affecting both men and women similarly.































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







