The document discusses post-obstructive diuresis (POD), which is a dramatic increase in urine output that can occur after relief of bilateral ureteral obstruction or obstruction of a solitary kidney. POD is a normal physiological response as the kidneys eliminate accumulated sodium, urea, and water. It is usually self-limiting as fluid and electrolyte homeostasis is regained. Pathological POD occurs if inappropriate fluid and solute excretion persists beyond the regained homeostasis state, requiring evaluation and management of fluid, electrolyte, and volume status.

![Pathologic POD secondary to salt-wasting
nephropathy: Dehydration and electrolyte
imbalance (Na+
, K+
, magnesium [Mg2+
]) are common as
the persistent natriuresis promotes the loss of water,
potassium and magnesium.
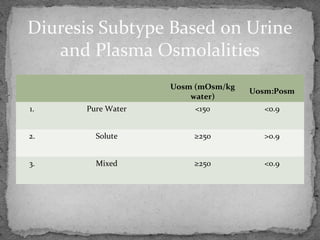
Urine osmolality (≥250 mOsm/kg water) is often
slightly higher than that of plasma.
Careful hemodynamic monitoring, CVP, frequent
monitoring of both serum and urine electrolytes.](https://image.slidesharecdn.com/postobstructivediuresis-170421132216/85/Post-obstructive-diuresis-16-320.jpg)