Downloaded 90 times


































































![• If a false passage is created, a retrograde study
[instilling contrast under continuous
fluoroscopy]
• if resistance is encountered and only
extravasation of contrast is seen, then it is
best not to pursue any further.](https://image.slidesharecdn.com/tipsandtrickssemirigidursfinal-181117215453/85/Tips-and-tricks-semirigid-urs-final-75-320.jpg)












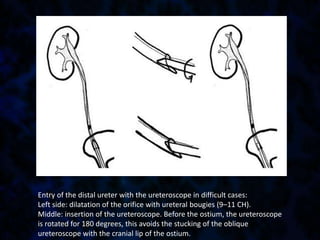
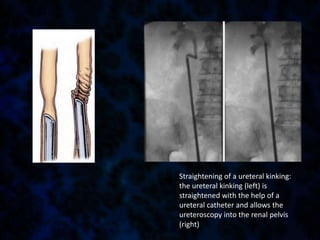
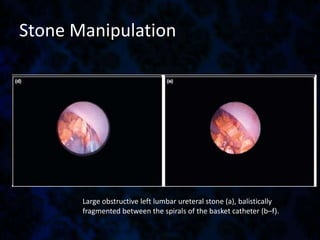
This document provides tips and tricks for performing semirigid ureteroscopy. It discusses preoperative preparation including reviewing imaging and planning the procedure. Patient positioning and access to the ureter are important considerations. Negotiating the ureteric orifice may require dilatation for difficult cases. Advancing the scope can be challenging in tortuous ureters and kinks may need to be straightened. Stone manipulation involves techniques to fragment and extract stones while preventing migration. Completing the procedure involves ensuring drainage with stenting when needed. Troubleshooting tips address problems that may arise like false passages or difficult baskets. Safety and recognizing complications early are emphasized.


















![Urology infection [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/urologyinfectionedmond-140716212859-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)




































































