Downloaded 98 times
![NIV in emergency department
Dr.Venugopalan.P.P
DA,DNB,MNAMS,MEM[GWU]
Director ,Emergency Medicine, Aster –DM health care
Site Director ,MEM program –GWU
Deputy Director –MIMS Academy
Founder and Executive Director -ANGELS
Emcon2014 Mumbai November 6 to 9](https://image.slidesharecdn.com/nivinemergencydepartmentebm-141109100155-conversion-gate01/85/Niv-in-emergency-department-ebm-1-320.jpg)
![NIV in emergency department
Dr.Venugopalan.P.P
DA,DNB,MNAMS,MEM[GWU]
Director ,Emergency Medicine, Aster –DM health care
Site Director ,MEM program –GWU
Deputy Director –MIMS Academy
Founder and Executive Director -ANGELS
Emcon2014 Mumbai November 6 to 9](https://image.slidesharecdn.com/nivinemergencydepartmentebm-141109100155-conversion-gate01/75/Niv-in-emergency-department-ebm-1-2048.jpg)
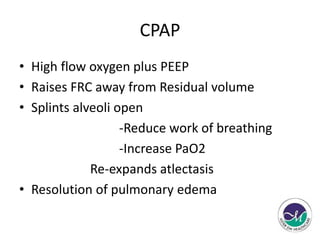
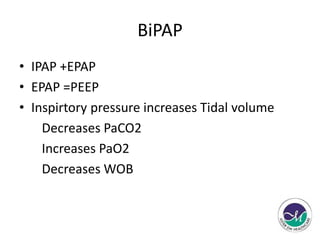
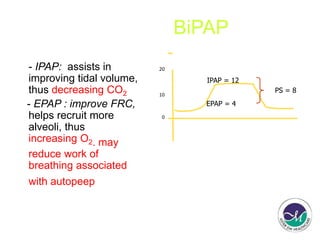
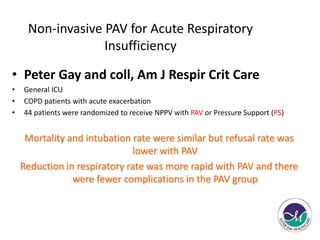
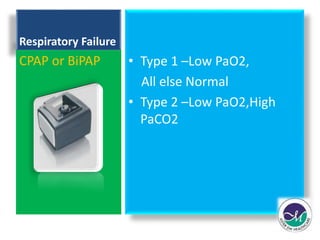
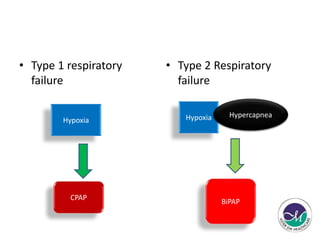




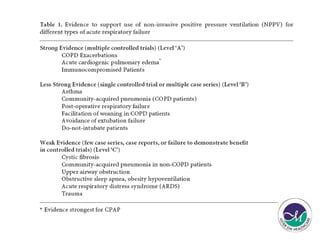
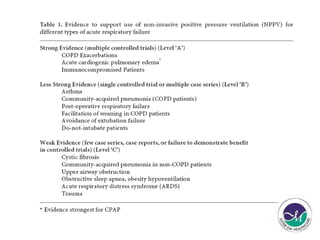
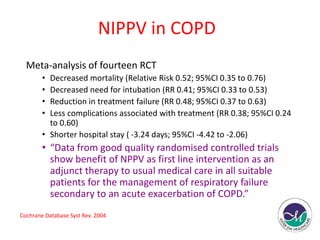
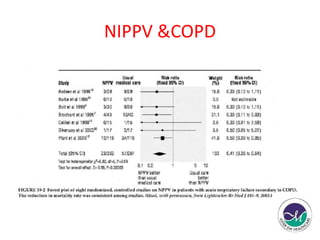
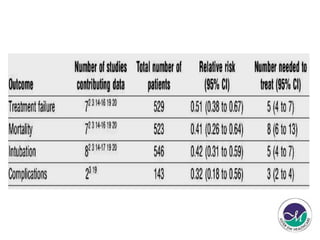
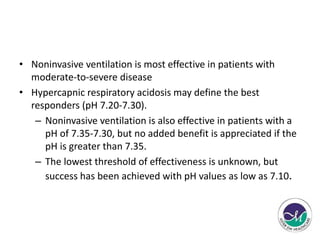
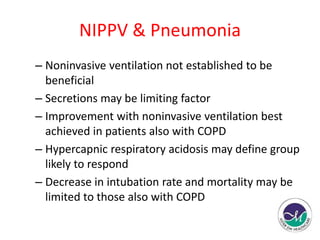


1) Noninvasive ventilation (NIV) refers to respiratory support provided without an endotracheal tube and allows spontaneously breathing patients. 2) NIV modalities like CPAP and BiPAP raise functional residual capacity and splint alveoli open, reducing work of breathing and increasing oxygen levels. 3) Studies show NIV effectively treats respiratory failure types 1 and 2, pulmonary edema, and as an adjunct in COPD exacerbations by decreasing intubation need, mortality, and length of stay. However, effectiveness in milder COPD, pneumonia, and asthma requires further research.























































































