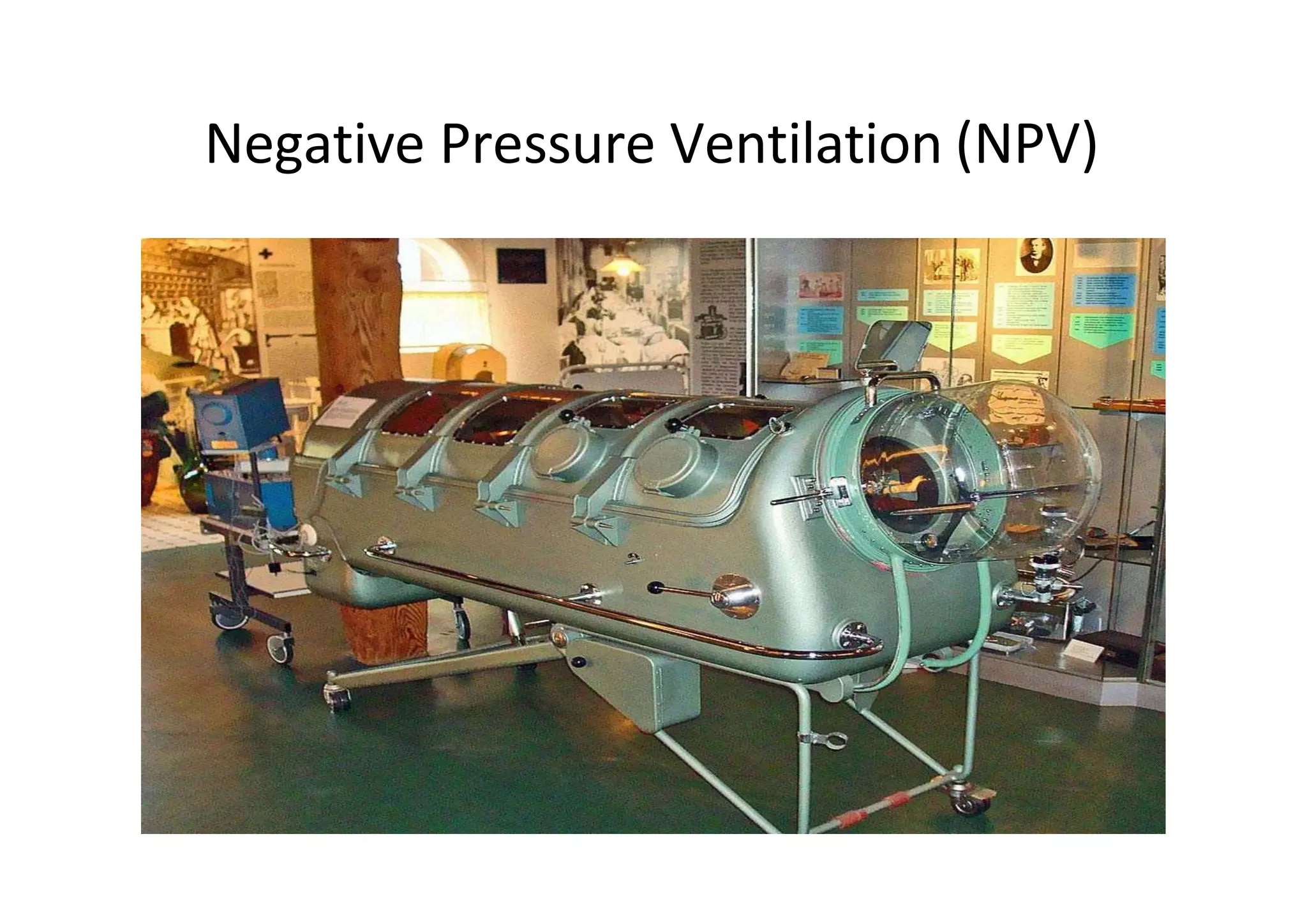
This document provides an overview of non-invasive ventilation (NIV), including its definition, types, advantages, indications, contraindications, interfaces, modes, guidelines for initiation and termination, and complications. NIV refers to mechanical ventilation without an invasive artificial airway and includes negative pressure ventilation techniques from the early 20th century as well as modern positive pressure methods like CPAP and BiPAP. NIV is advantageous for avoiding intubation risks while still providing ventilatory support. It is indicated for respiratory conditions like COPD exacerbations and acute pulmonary edema. Careful patient selection and monitoring is required for safe and effective NIV use.